⏱ 9 min read
A 2026 SEEearly baseline report found that 53.3% of 184 young people with early schizophrenia-spectrum psychosis were not in employment, education, or training at study entry, even though 97.8% had at least a lower- or upper-secondary school-leaving qualification.1 Psychosis had already interrupted the bridge from school into training, college, or competitive work.
Research Highlights
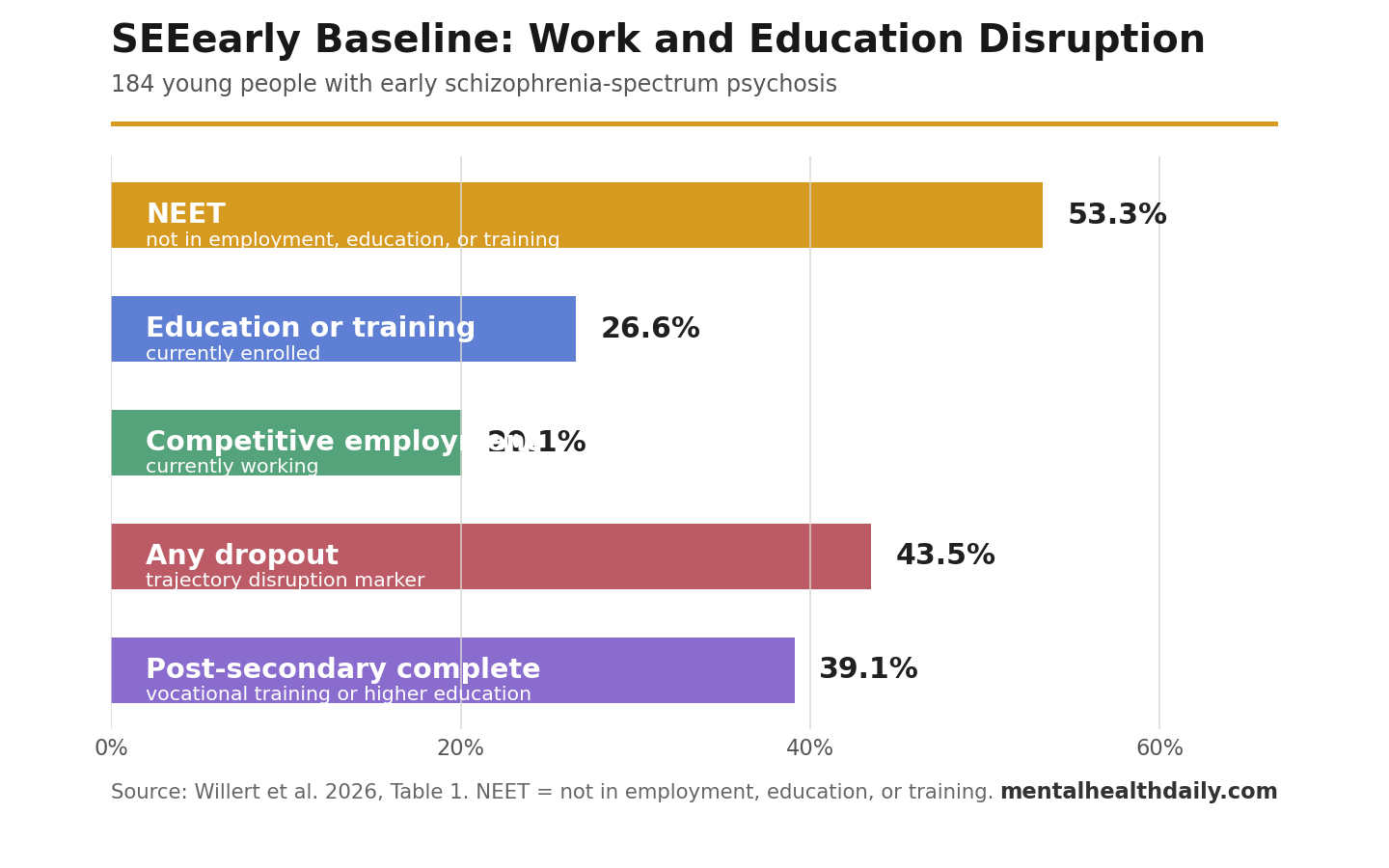
- NEET status was the headline finding: 98 of 184 participants (53.3%) were not in employment, education, or training before randomization in the SEEearly trial.1
- School completion did not prevent disruption: 97.8% had at least ISCED level 2 or 3 school-leaving qualification, but only 39.1% had completed vocational training or higher education.1
- Only a minority were currently attached to work or school: 20.1% were competitively employed and 26.6% were in education or training at baseline.1
- Dropout history was common: 43.5% had at least 1 dropout, and 67.8% lived on less than 1000 euros per month.1
- The paper is baseline calibration, not an outcome result: SEEearly had not yet tested the intervention effect; it showed why supported employment and education should measure school, training, and maintained participation, not job status alone.1
Supported employment and education means practical help with competitive work, mainstream education, and training while psychiatric care continues. The strongest version comes from individual placement and support (IPS), a model that tries to move people quickly toward real jobs or school roles based on their preferences rather than waiting for symptom remission first.
In early psychosis, that target belongs near the center of care. Adolescence and young adulthood are exactly when people finish secondary school, start apprenticeships, enter college, build early work histories, and avoid the first long gaps that can harden into future exclusion.
SEEearly Enrolled 184 Young People With Schizophrenia-Spectrum Psychosis
Willert et al. described the baseline cohort entering SEEearly, a six-site German randomized trial testing supported employment and education plus treatment as usual vs. treatment as usual alone. Participants were 16 to 35 years old, had early psychosis within the past 5 years, met DSM-5 criteria for a schizophrenia-spectrum or other psychotic disorder, and expressed interest in competitive employment or mainstream education.1
Baseline report: the paper did not report whether SEEearly worked. Randomization came after baseline assessment, and the article’s value is the intake profile: who entered the trial, how disrupted their education and work paths already were, and how the cohort compared with earlier employment and education trials.
Recruitment was selective in clinically important ways. The study screened 446 people from October 2022 through December 2024, excluded 259, and randomized 184 after baseline. Exclusion most often reflected failure to meet early psychosis criteria (127 people) or lack of interest in participation (112 people). Participants also needed at least A2 German language ability and enough functional capacity to engage with mainstream work or education goals.
53.3% Were Out of Employment, Education, or Training
NEET means not in employment, education, or training. It is a blunt status marker, but in early psychosis it captures a real functional risk: a young person can be clinically engaged with services while already losing time in the education-to-work sequence.
At SEEearly intake, 98 participants were NEET (53.3%). Only 37 participants were in competitive employment (20.1%), and 49 were in education or training (26.6%). That pattern is worse than a simple unemployment statistic because the study age range includes people who should reasonably be in school, vocational training, or early career entry rather than full-time work alone.
The education numbers sharpen the point. Nearly all participants had at least lower- or upper-secondary school-leaving qualification: 63 had ISCED level 2, 117 had ISCED level 3, and only 4 had no school-leaving qualification or primary-level education. Yet only 72 participants (39.1%) had completed vocational training or higher education.
School-Leaving Qualification Was Not the Same as Vocational Recovery
The useful concept in this paper is vocational trajectory: the sequence from school completion into training, college, competitive employment, and sustained participation. A snapshot of current employment can miss earlier breaks in that sequence.
SEEearly makes that visible. School-leaving qualification was common, but post-secondary completion was low, and participants with completed vocational training or higher education were older than those without a degree (29.2 vs. 23.5 years). The study team also reported that almost half of those without any degree, and almost half of those with secondary qualification, belonged to the NEET group.
Dropout signal: 80 participants (43.5%) had at least 1 dropout. That is the kind of functional marker that can appear before a clean diagnostic endpoint, and it is exactly why employment-only outcomes understate the problem in young psychosis cohorts.
Financial data pointed in the same direction. Only 21.7% earned income from competitive employment, 30.4% received social security benefits or educational loans, 46.7% relied on other sources such as family, and 67.8% lived below the study’s 1000-euro monthly threshold for available subsistence.
The Cohort Was Diagnostically Narrower Than Many Earlier Trials
SEEearly differed from broad severe-mental-illness employment studies by using a diagnostically narrower psychosis cohort. All 184 participants had a schizophrenia-spectrum diagnosis: schizophrenia in 52.7%, brief psychotic disorder in 16.8%, schizoaffective disorder in 14.7%, unspecified schizophrenia-spectrum disorder in 8.7%, schizophreniform disorder in 4.3%, other specified psychotic disorder in 2.2%, and delusional disorder in 0.5%.
Clinical severity: Positive and Negative Syndrome Scale (PANSS) total score averaged 57.4. PANSS is a clinician-rated symptom scale for psychosis in which higher scores indicate more severe positive symptoms, negative symptoms, and general psychopathology. Global Assessment of Functioning (GAF), a broad functioning score where higher is better, averaged 57.8. Substance misuse was present in 44.6%.
Compared with earlier supported employment and education trials, SEEearly had larger sample size than the psychosis-only Killackey 2008 and Nuechterlein 2020 studies, and it was more diagnostically homogeneous than trials mixing psychotic disorders with mood disorders.34
IPS and SEE Evidence Already Supports Work-or-School Outcomes
Early intervention services for psychosis outperform usual care across several clinical and functional outcomes in meta-analysis, but symptom improvement does not automatically rebuild a vocational path.2 That is where IPS and supported education models enter the picture.
Killackey et al. tested individual placement and support for vocational recovery in first-episode psychosis and reported better vocational outcomes than treatment as usual.3 Nuechterlein et al. tested IPS plus workplace fundamentals training after a first episode of schizophrenia, making return to work or school the actual recovery target rather than a vague quality-of-life add-on.4
Education-sensitive recovery: a school-age or early-adult cohort needs different endpoints than a midlife employment program. Returning to college, staying in vocational training, avoiding repeated dropout, completing a credential, and maintaining competitive work are different milestones. SEEearly’s baseline paper argues for measuring that sequence directly.
NEET Status Is a Warning Marker, Not the Whole Mechanism
Maraj et al. described the “NEET trap” in early intervention psychosis care: vocational inactivity and disengagement from services can cluster together, making recovery harder to restart once the person falls outside both school/work and care routines.5 SEEearly adds a cleaner diagnostic intake profile to that concern.
Still, NEET status should not be treated as a causal explanation by itself. A person can be NEET because of active positive symptoms, negative symptoms, cognitive impairment, sedation, substance misuse, family disruption, stigma, language barriers, poverty, fear of relapse, lack of flexible schooling, or loss of confidence after hospitalization.
Useful assessment separates those drivers:
- Symptom barrier: hallucinations, paranoia, disorganization, depression, anxiety, or negative symptoms directly block attendance or performance.
- Cognitive barrier: attention, working memory, processing speed, or planning problems make school and job demands harder.
- Systems barrier: services focus on medication and relapse prevention while school accommodations, benefits counseling, and employer contact arrive late.
- Trajectory barrier: a dropout, failed apprenticeship, or prolonged absence creates a gap that becomes harder to explain and repair over time.
Supported employment and education is strongest when it treats those barriers as practical problems to solve while psychiatric treatment continues.
Baseline Data Cannot Prove SEEearly Works
This paper’s limit is straightforward: no intervention effect was tested. It cannot say whether supported employment and education increased school participation, employment, credential completion, income, symptoms, quality of life, or service engagement over 12 months.
Selection limits: participants had to want competitive employment or mainstream education, speak enough German, and be able to participate in the trial. The study also overrepresented metropolitan German sites and included no site in the eastern federal states. Those choices improve trial feasibility but narrow generalizability.
Best use of the finding: clinicians and service planners should not wait for symptom remission before tracking school and work recovery. A young person with early psychosis can have completed school, remain interested in work, and still be sliding into a NEET trajectory that needs direct intervention.
Questions About Early Psychosis and Vocational Recovery
Does this SEEearly paper prove that supported employment and education works?
No. It reports baseline characteristics before treatment outcomes. The trial’s later follow-up will be needed to test whether SEE plus treatment as usual outperforms treatment as usual alone.
Why is 53.3% NEET status important?
It shows that more than half the cohort was already outside work, school, or training at study entry. In a 16- to 35-year-old early psychosis sample, recovery planning has to include school and training pathways alongside symptom reduction.
Why is employment alone too narrow?
Employment alone misses younger participants who should be in education or vocational training. A person can be on a healthy recovery path without a job if they are completing school, and a person can be at serious risk if repeated education disruptions block future employment.
Who does this evidence apply to?
The most direct application is young people with early schizophrenia-spectrum psychosis who want mainstream work or education and are clinically able to engage with a supported employment and education program. It should not be generalized to every person with psychosis regardless of phase, language, medical disability, or service context.
What should early psychosis services measure?
Services should track current work or school status, dropout history, credential completion, income source, benefit concerns, cognitive barriers, symptom barriers, and whether the person is maintaining participation over time. A single job-status field is too thin for this age group.
References
- Baseline Characteristics of a Diagnostically Defined Early Psychosis Cohort Entering Supported Employment and Education: Findings From the SEEearly Trial. Willert A et al. European Archives of Psychiatry and Clinical Neuroscience. 2026. doi:10.1007/s00406-026-02236-8
- Comparison of Early Intervention Services vs Treatment as Usual for Early-Phase Psychosis: A Systematic Review, Meta-Analysis, and Meta-Regression. Correll CU et al. JAMA Psychiatry. 2018;75(6):555-565. doi:10.1001/jamapsychiatry.2018.0623
- Individual Placement and Support for Vocational Recovery in First-Episode Psychosis: Randomised Controlled Trial. Killackey E et al. British Journal of Psychiatry. 2019;214(2):76-82. doi:10.1192/bjp.2018.191
- Enhancing Return to Work or School After a First Episode of Schizophrenia: The UCLA RCT of Individual Placement and Support and Workplace Fundamentals Module Training. Nuechterlein KH et al. Psychological Medicine. 2020;50(1):20-28. doi:10.1017/S0033291718003860
- Caught in the “NEET Trap”: The Intersection Between Vocational Inactivity and Disengagement From an Early Intervention Service for Psychosis. Maraj A et al. Psychiatric Services. 2019;70(4):302-308. doi:10.1176/appi.ps.201800118
Leave a Reply