Main
Autism spectrum disorders, henceforth ‘autism’, are a set of early onset neurodevelopmental conditions characterized by differences in sociocommunicative abilities and rigid and repetitive behaviors and interests1. Autism is a lifelong condition and has a global prevalence of approximately 1%2. While not a part of diagnostic criteria, autistic people across the lifespan often have co-occurring mental health difficulties3,4,5,6,7, with systematic reviews finding prevalence rates of 20–23% (current) and 42% (lifetime) for anxiety disorders8,9. Notably, anxiety has been identified as one of the top two priorities in autism research by autistic people themselves10. While anxiety has been well studied in younger autistic populations3,4, only a small number of studies have specifically examined the rates of anxiety diagnoses5,6,7,11,12 and prevalence of anxiety symptoms6,7,13,14,15,16,17 in middle-aged and older people on the autism spectrum. As such, our current understanding of the burden and course of anxiety in autistic populations in midlife and older age is limited.
At present, only one follow-up study has examined mental health changes in middle aged and older autistic adults18. Over an average follow-up period of 2.4 years, the study found no significant change in anxiety symptoms. However, the short follow-up window limits conclusions about longer-term trajectories associated with aging. Cross-sectional studies provide mixed evidence regarding the rates of anxiety across different age groups in autism. There has been evidence to suggest lower rates of clinical anxiety in older autistic populations compared to younger autistic age groups19, while other studies have found the opposite pattern20. Still other studies identify complex age associations, such as cubic trends where symptoms decrease in younger adulthood and resurge in midlife21 or no significant differences across the lifespan altogether22. These inconsistencies, coupled with the limitations of cross-sectional designs and potential cohort effects, underscore the need for more longitudinal research to clarify developmental patterns in anxiety across the adult lifespan in autism.
There are two main issues that surface when trying to address this gap. The first is the issue of underdiagnosis among those who are middle-aged and older. Estimates suggest that nine out of every ten autistic adults in this age range are undiagnosed23,24, which is probably the result of the changes to the diagnostic criteria and conceptualization of autism in the past 50 years25,26. This impedes recruitment of middle-aged and older autistic people with a diagnosis to research studies. A trait-based approach offers a valuable alternative to diagnosis-based recruitment, particularly in midlife and older populations where autism is frequently underrecognized or misdiagnosed27. This approach allows researchers to identify people with elevated autistic traits and characteristics who may not have received a formal diagnosis, thus capturing a broader and potentially more representative sample of autistic adults.
The second consideration is the heterogeneity associated with the longitudinal course of anxiety between individuals28, which standard repeated-measure analyses cannot capture. This has been addressed in general population studies using longitudinal forms of latent class analysis and growth mixture modeling (GMM) methods. These statistical procedures allow the modeling of individual trajectories of a given outcome and the subsequent identification of previously unobserved subpopulations within a heterogeneous sample29.
The aim of the current study is to use GMM to identify distinct anxiety trajectories in a large, longitudinal cohort of middle-aged and older adults and examine whether endorsement of sociocommunicative autistic traits is associated with trajectory class membership. These results could provide insight into the experience of aging with autism and improve understanding of the mental health support needs of this understudied population.
Results
Demographics and lifetime psychiatric diagnoses
All descriptive statistics for the overall sample and by group and are presented in Table 1. The majority of the sample reported their biological sex as female (75%), and there was an underrepresentation of Black, Asian and Minority Ethnic (BAME) people (1.3%) compared with the general population. The median age at baseline was 62 years. While age, gender ratio and ethnicity did not differ between the autism spectrum trait (AST) and comparison adults (COA) groups, higher baseline depression scores (Patient Health Questionnaire-9, PHQ-9) were observed in the AST group. However, prevalence rates of lifetime diagnoses of major depressive disorder and generalized anxiety disorder did not differ between groups. By contrast, larger proportions of the AST group reported having lifetime diagnoses of social anxiety, panic disorder and obsessive–compulsive disorder (OCD). Furthermore, no participant in the overall sample had an autism diagnosis.
Using a subsample of the full PROTECT cohort with sufficient longitudinal data for GMM analysis (that is, at least baseline plus two annual follow-up assessments), a total sample of 5,270 participants (n = 3,955 female; 75.0%) was included in the analyses, of whom 66 (1.25%) met cutoff criteria for the high AST group (see ‘Measures’ section in the Methods for inclusion criteria). Participants who were found to endorse no traits using this measure formed the COA group (n = 3,874, 73.51%). Participants with missing scores (n = 237, 4.50%) and those who endorsed some traits but fell below the cutoff (n = 1,093, 20.74%) were also included in the GMM to maximize statistical power and trajectory identification but were excluded from further analyses (Table 2).
Model selection
Comparison of one-class growth models revealed that a quadratic GMM provided better fit than a linear model (Supplementary Tables 1–4). However, it was found that quadratic models with three or more classes were converging on improper solutions, as the estimated correlation between the linear and quadratic slopes was almost perfectly negative in both cases. The variance of the quadratic term was also very small, which made the models susceptible to instability during estimation. To address this, the variance of the quadratic term was fixed to be 0.
Trajectories of anxiety symptoms change for total sample
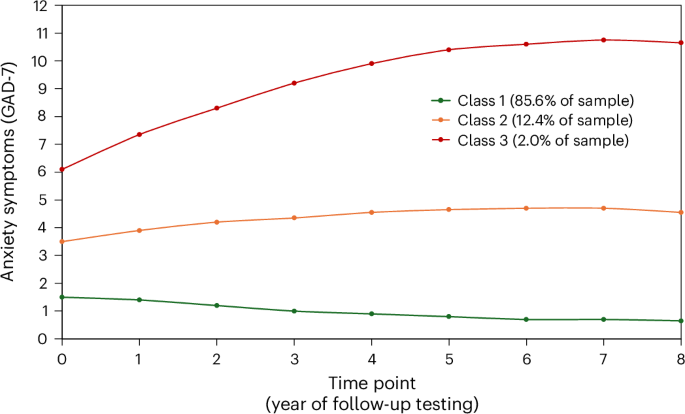
GMM analysis was conducted on the entire sample (n = 5,270; AST 66, COA 3,874, missing AST score 1,330). Overall, a three-class model was selected as the final model (see Supplementary Tables 1–4 for model fit statistics and Supplementary Table 5 for class-stratified demographics). While the Akaike information criterion (AIC), Bayesian information criterion (BIC) and sample-size-adjusted BIC (ABIC) values were lower for the three-class model, the adjusted Lo–Mendel–Rubin (LMR) and adjusted likelihood ratio test (ALRT) indices were no longer significant in the three-class model. These metrics can be sensitive to sample size and may not detect small but meaningful classes. As such, we prioritized the three-class model based on AIC, BIC, ABIC and interpretability, and because it captured a distinct subgroup of 56 people (1.06% of the full sample) with clinically significant anxiety trajectories, a trajectory not identified in the two-class model. For the same reason, models with more than three classes were not considered. As estimated prevalence rates of anxiety disorders in older adult community samples range from 1.2% to 15%30, we opted to retain this class. The identified trajectories are shown in Fig. 1 and were described on the basis of standard Generalized Anxiety Disorder-7 (GAD-7) symptom thresholds31: ‘class 1’, lower-range minimal anxiety; ‘class 2’; upper-range minimal anxiety; and ‘class 3’, mild-to-clinical anxiety.
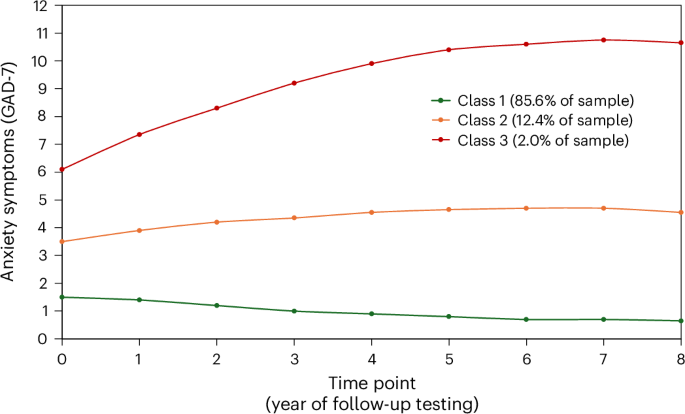
A three class model, with ‘class 1’ representing lower-range minimal anxiety, ‘class 2’ representing upper-range minimal anxiety and ‘class 3’ representing mild-to-clinical anxiety.
Class 1 was the largest trajectory class, comprising 85.6% of the sample. People in this class were characterized by estimated GAD-7 scores ranging from 0.5 to 1.5 over the eight years, remaining at the lower end of the ‘minimal anxiety’ range (scores 0–4)32. Membership in this class was more frequently observed in the COA group (88.2%), compared with the AST group (57.58%). Class 2 consisted of 12.4% of the total sample and showed anxiety scores that persisted in the upper end of what is labeled ‘minimal anxiety’. The reverse pattern to class 1 is seen here, in that a greater proportion of the AST group were represented by this class (30.3%) compared with the COA group (19.56%). Class 3, the smallest of the three trajectories identified, 2%, was the only class to show a notable change in anxiety, with scores gradually rising from mild to clinical levels over time. Again, it was more common for AST participants to belong to this class (12.12%) than the COA participants (1.24%).
Associations between sociocommunicative autistic traits and class membership were investigated using unadjusted (Table 3) and adjusted (Tables 4 and 5) multinomial logistic regression models, using class 1 (lower-range minimal anxiety) as the reference group. In the unadjusted model, AST participants had 4.40 times the relative risk (RR) of belonging to class 2 (versus class 1), and 15.00 times to the RR of belonging to class 3 (versus class 1) compared with COA participants. This effect remained consistent when adjusting for sex and age (Table 4). While the effect size was attenuated when adjusting for baseline depression (PHQ-9), AST participants were still at significantly greater likelihood of belonging to class 2 and more so class 3 than COA participants.
Discussion
This study provides longitudinal evidence that the heightened risk of anxiety faced by those with elevated autistic traits persists into midlife and older age. In our sample of over 5,200 middle-aged and older adults, we identified three trajectories of anxiety symptoms over an 8-year period. The two largest classes (class 1: 85.6% of sample, class 2: 12.4% of sample) were characterized by anxiety scores within the minimal symptom range (0–5) of the commonly used anxiety symptom measure, the GAD-7. Although these two classes were identified as having distinct probabilities of anxiety, due to their low scores, they are unlikely to be differ greatly in terms of clinical presentation. The third and smallest class (class 3: 2% of sample) showed a curved anxiety trajectory where scores gradually increased from mild to clinical anxiety over the eight annual time points studied. Although this class comprised only 2% of the sample, given the large total sample size, robust detection of distinct, smaller classes was feasible. These findings are consistent with previous GMM studies in general population samples that have also identified small class sizes in mental health trajectories33,34.
When considering the distribution of the high autistic trait (AST) and low autistic trait comparison (COA) groups, we found these to vary in proportion across classes. A greater proportion of AST participants were classified into class 3 (mild-to-clinical trajectory; AST 12.12%, COA 1.24%) and class 2 (upper-range minimal anxiety trajectory; AST 30.30%, COA 10.56%), whereas most COA participants were classified into class 1 (lower-range minimal anxiety; AST 57.58%, COA 88.20%). Although members of the AST group were found across all three classes, multinomial logistic regression showed that, relative to class 1, AST participants were upward of 14 times more likely to belong to class 3 than COA participants, an effect that remained after adjusting for depression scores, although attenuated. This suggests that some middle-aged and older people with high autistic traits are more susceptible to high and persistent anxiety than their low-trait peers.
The finding that the AST group was overrepresented in class 3 aligns with the findings from both cross-sectional studies5,7 and the only other longitudinal follow-up study of mental health in ageing in relation to autism18, which similarly found that high levels of anxiety were sustained over time. However, our use of GMM revealed a steady increase from subclinical to clinical GAD-7 scores (≥10) observed in class 3, highlighting the need for early intervention strategies for anxiety. Indeed, previous research has demonstrated that treatment of mild psychological disorders can significantly reduce the proportion of future more severe cases35. Adapted forms of low-intensity cognitive behavioral therapy have proved successful for mild-to-moderate depression in autistic adults36, suggesting the potential for similar approaches in addressing subclinical anxiety.
There are several possible reasons why some middle-aged and older adults with elevated autistic traits might face an increased risk for greater anxiety. Studies have found that autistic traits are associated with an increased risk of experiencing loneliness and isolation13, trauma across the lifespan, and the impact of severe trauma on PTSD symptoms15,37,38,39. Autistic people are also more likely to experience barriers in health care services, so they may be less likely to receive appropriate treatment for anxiety40,41,42,43. A lifetime of these adverse experiences is likely to contribute to discrepancies in mental health difficulties faced by autistic and non-autistic adults beyond midlife.
It will be important to consider how the barriers to receiving mental health care for autistic people (for example, communication difficulties and limited specialized knowledge of mental health in aging with autism) will be compounded with other upper-age barriers (for example, stigma around mental illness that prevents help-seeking)44. Autism and mental health research must therefore consider this intersectionality going forward. In addition, it is important to consider the specificity of these findings; for example, are these experiences and patterns unique to autistic populations, or are they also observed in other neurodivergent groups (for example, people with attention deficit hyperactivity disorder) or in individuals with long-term disabilities and health conditions? Cross-group comparative studies would facilitate this type of exploration and should be considered in future research.
Limitations and strengths
It will also be important to consider the present findings in light of the following limitations. First, the current study was not preregistered. Second, as PROTECT is an ongoing study, baseline is tied to the point of entry for each participant. Consequently, these trajectories cannot be localized to a certain age range. Also, this study excluded participants who took part in fewer than three time points, the minimum requirement for estimation of GMMs45. However, people with psychiatric disorders often show higher attrition46 and therefore may not be fully represented in this study. Diversity and representation were also limited by the demographic characteristics of the PROTECT sample, which is predominately made up of white, female, well-educated participants, with no BAME people in the AST group at all. However, this issue is not unique to the PROTECT cohort and is common in both aging and autism research fields47,48. It is also worth noting that anxiety is often more common in women than men49. Our class 2 and 3 groupings did have significantly more women than men in them, which aligns with these anxiety sex/gender differences observed in the general population. As such, given the overrepresentation of individuals of white ethnicity and females in our sample, future research should seek to replicate these findings in ethnically diverse and sex- and gender-balanced samples. Also, consideration should specifically be given to middle-aged and older BAME autistic people as studies like ours may not be representative of their experiences. Furthermore, a final point to consider is that the AST group was relatively small, particularly in the mild-to-clinical trajectory; this may reduce statistical precision, and as such, the results should be interpreted in this context. Replication of these findings in larger samples of diagnosed autistic people would be valuable.
However, there are notable strengths in the current study. Although the AST sample was small and derived from a brief screener (which focuses on sociocommunicative difficulties but has good sensitivity and specificity for identifying autistic individuals), it represented only 1.3% of the overall sample. Although we cannot confirm whether these identified high autistic trait participants would meet diagnostic criteria for autism, the overall group proportion identified aligns with epidemiological estimates of autism within the general population (~1%)2,23. In addition, the overall sample of 5,270 allows robust GMM estimation. Furthermore, the number of classes included in the final GMM was driven by the data (rather than an a priori decision). The iterative process used in GMM supported the three-class model. However, this solution should be interpreted with some caution, given mixed fit indices and the relatively small size of class 3. The high entropy suggests good classification accuracy for the three-class model. We note that that this autistic-trait-based work should be replicated using more diverse samples, including those with a diagnosis of autism, intellectual disabilities and different cultural and ethnic contexts. This will allow a more comprehensive understanding of the risk of anxiety in this population.
Conclusion
Three distinct anxiety trajectories were identified in this large general population sample of middle-aged and older adults. Participants with elevated sociocommunicative autistic traits were found to be at a greater risk of experiencing higher anxiety symptoms over time. Given the detrimental consequences of chronic anxiety for physical and mental health, these findings highlight the need for increased, tailored support for adults on the autism spectrum. Researchers, clinicians and health policymakers should aim to collaborate with autistic people where possible, as their lived experience affords vital insight into their support needs during the transition into midlife and older age.
Methods
Study design and participants
The present study uses 8 years of annual longitudinal data from the PROTECT study (www.protectstudy.org.uk). PROTECT is an ongoing, online research study with annual follow-ups based in the UK that aims to examine aging and health. The PROTECT study uses a wide range of recruitment methods, including public and national press and radio, as well as established aging research networks. Potential participants are directed to register online via the PROTECT platform and are required to review an information sheet and to provide informed consent to take part. Participants are required to meet the following inclusion criteria for the PROTECT study: be at least 40 years of age (due to the focus on mid-to-late life), have a working proficiency of the English language, be a resident of the UK and have access to a device with Internet access. The only two exclusion criteria for the PROTECT study are: having a dementia diagnosis at baseline assessment and being unable to consent.
The PROTECT study was piloted in 2014 and publicly commenced in 2015. As an ongoing study, baseline is defined as each participant’s point of entry and is not study specific. Participants receive annual follow-up requests for participation via email. While the present study is an analysis of up to eight consecutive years of assessment, those who joined PROTECT in more recent years have fewer time points of annual follow-ups.
Ethical approval for the PROTECT study was obtained from the London Bridge National Research Ethics Committee (reference 13:/LO/1578).
Measures
Demographic information and medical history
All participants who participated in the PROTECT study completed an online demographic information questionnaire at baseline, which collected data including participants’ age, sex, ethnicity and several lifetime psychiatric diagnoses (major depressive disorder, generalized anxiety disorder, panic disorder, social anxiety and OCD; Table 1).
Autistic traits
The present study used the bespoke PROTECT Autistic Traits measure, which is a five-item screener that assesses childhood and current sociocommunicative autistic traits7. This measure was completed at baseline. Using a yes/no format, the participant was asked if as a child they had “struggled compared to [their] peers (socially or at school) with: (1) knowing how to get along with other children; (2) understanding other kids’ jokes, sarcasm or deception.” Further questions asked if the participant “currently find[s] it more difficult than other people to: (1) make and keep friends; (2) understand other people’s perspectives; (3) recognize if someone means something different from what they are saying.” To meet the cutoff for the AST group, participants needed to endorse both childhood traits and at least two of the three current traits. Those who did not endorse any past or present autistic traits formed the COA group.
The PROTECT Autistic Traits measure has been found to have high sensitivity (82%) and specificity (96%) for identifying people with an autism diagnosis, good convergent validity with other widely used autistic trait measures (that is, the AQ-1050 and RAADS-1451) and very good internal consistency (Cronbach’s α = 0.82)7.
Self-report questionnaire measures
GAD-731 is a widely used seven-item questionnaire that assesses symptoms of anxiety experienced in the past 2 weeks. Using the standard cutoff of ≥10, the GAD-7 has a sensitivity of 89% for identifying people with generalized anxiety disorder. Recent symptoms of major depressive disorder were measured using PHQ-952, a nine-item measure, with a cutoff for clinical cases of ≥10. The GAD-7 and PHQ-9 were completed at baseline and at each annual follow-up entry.
Plan of analysis
GMM was used to estimate trajectories of anxiety symptoms over the eight waves of testing (using data collected at baseline then at each subsequent annual follow-up entry). Anxiety (GAD-7) scores from all participants (that is, n = 5,270) were included in the estimation to maximize sample size. Linear and quadratic growth models were compared to determine which provided a better fit to the data. Models with increasing numbers of classes were estimated and compared.
As there were no prior hypotheses about the number of classes, quadratic GMMs with K classes were sequentially compared with K − 1 classes. Several relative fit information criteria are available for consideration when comparing GMMs. These include the AIC, the BIC, the ABIC, the entropy, the Vuong–Lo–Mendell–Rubin test, and adjusted LMR and ALRT tests. The proportion of the smallest group was also considered. All GMM analyses were conducted using Mplus 8.153.
Multinomial logistic regression models unadjusted and adjusted for demographic characteristics and depression were run using Stata version 1754 to assess the association between sociocommunicative autistic traits and class membership.
Missing data
Participants who had total GAD-7 scores for fewer than three time points (that is, baseline plus two annual follow-up entries) were excluded from GMM analysis, as this is the recommended minimum requirement for proper estimation of GMMs45. Full information maximum likelihood was used to handle missing data on GAD-7 scores.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Due to data access and sharing restrictions, the data used in this study are not publicly available. For further information about data access, please contact the corresponding authors.
References
-
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR (American Psychiatric Association Publishing, 2022); https://doi.org/10.1176/appi.books.9780890425787
-
Santomauro, D. F. et al. The global epidemiology and health burden of the autism spectrum: findings from the Global Burden of Disease Study 2021. Lancet Psychiatry 12, 111–121 (2025).
-
Vasa, R. A., Keefer, A., McDonald, R. G., Hunsche, M. C. & Kerns, C. M. A scoping review of anxiety in young children with autism spectrum disorder. Autism Res. 13, 2038–2057 (2020).
-
Nimmo-Smith, V. et al. Anxiety disorders in adults with autism spectrum disorder: a population-based study. J. Autism Dev. Disord. 50, 308–318 (2020).
-
Lever, A. G. & Geurts, H. M. Psychiatric co-occurring symptoms and disorders in young, middle-aged, and older adults with autism spectrum disorder. J. Autism Dev. Disord. 46, 1916–1930 (2016).
-
Stewart, G. R. et al. The mental and physical health of older adults with a genetic predisposition for autism. Autism Res. 13, 641–654 (2020).
-
Stewart, G. R. et al. The mental and physical health profiles of older adults who endorse elevated autistic traits. J. Gerontol. B. https://doi.org/10.1093/geronb/gbaa112 (2020).
-
Hollocks, M. J., Lerh, J. W., Magiati, I., Meiser-Stedman, R. & Brugha, T. S. Anxiety and depression in adults with autism spectrum disorder: a systematic review and meta-analysis. Psychol Med. 49, 559–572 (2019).
-
Lai, M. C. et al. Prevalence of co-occurring mental health diagnoses in the autism population: a systematic review and meta-analysis. Lancet Psychiatry 6, 819–829 (2019).
-
Benevides, T. W. et al. Listening to the autistic voice: mental health priorities to guide research and practice in autism from a stakeholder-driven project. Autism 24, 822–833 (2020).
-
Hand, B. N., Angell, A. M., Harris, L. & Carpenter, L. A. Prevalence of physical and mental health conditions in Medicare-enrolled, autistic older adults. Autism 24, 755–764 (2020).
-
Croen, L. A. et al. The health status of adults on the autism spectrum. Autism 19, 814–823 (2015).
-
Stewart, G. R., Luedecke, E., Mandy, W., Charlton, R. A. & Happé, F. Experiences of social isolation and loneliness in middle-aged and older autistic adults. Neurodiversity 2, 27546330241245529 (2024).
-
Stewart, G. R. et al. Sleep problems and mental health difficulties in older adults who endorse high autistic traits. Res. Autism Spectr. Disord. 77, 101633 (2020).
-
Stewart, G. R. et al. Traumatic life experiences and post-traumatic stress symptoms in middle-aged and older adults with and without autistic traits. Int. J. Geriatr. Psychiatry 37, gps.5669 (2022).
-
Chen, Y. et al. “Utterly overwhelming”—a mixed-methods exploration of sensory processing differences and mental health experiences in middle-aged and older autistic adults. Autism Adulthood https://doi.org/10.1089/aut.2024.0031 (2024).
-
Roper, S. et al. Sleep problems and mental health in middle-aged and older autistic and non-autistic adults. Preprint at Research Square https://doi.org/10.21203/rs.3.rs-7677602/v1 (2025).
-
Roestorf, A., Howlin, P. & Bowler, D. M. Ageing and autism: a longitudinal follow-up study of mental health and quality of life in autistic adults. Front. Psychol. 13, 741213 (2022).
-
Yarar, E. Z. et al. Aging and autism: do measures of autism symptoms, co-occurring mental health conditions, or quality of life differ between younger and older autistic adults? Autism Res. 15, 1482–1494 (2022).
-
Roy, M., Prox-Vagedes, V., Ohlmeier, M. D. & Dillo, W. Beyond childhood: psychiatric comorbidities and social background of adults with Asperger syndrome. Psychiatr. Danub. 27, 50–59 (2015).
-
Davis, T. E. et al. Anxiety symptoms across the lifespan in people diagnosed with autistic disorder. Res. Autism Spectrum Disord. 5, 112–118 (2011).
-
Uljarević, M. et al. Anxiety and depression from adolescence to old age in autism spectrum disorder. J. Autism Dev. Disord. 50, 3155–3165 (2020).
-
O’Nions, E. et al. Autism in England: assessing underdiagnosis in a population-based cohort study of prospectively collected primary care data. Lancet Reg. Health Eur. 29, 100626 (2023).
-
Stewart, G. R. & Happé, F. Aging across the autism spectrum. Annu. Rev. Dev. Psychol. 7, 4.1–4.24 (2025).
-
Lai, M. C. & Baron-Cohen, S. Identifying the lost generation of adults with autism spectrum conditions. Lancet Psychiatry 2, 1013–1027 (2015).
-
Happé, F. & Frith, U. Annual Research Review: looking back to look forward – changes in the concept of autism and implications for future research. J. Child Psychol. Psychiatry 61, 218–232 (2020).
-
Happé, F. & Frith, U. Dimensional or categorical approaches to autism? Both are needed. A reply to Nick Chown and Julia Leatherland. J. Autism. Dev. Disord. 51, 752–753 (2021).
-
Nandi, A., Beard, J. R. & Galea, S. Epidemiologic heterogeneity of common mood and anxiety disorders over the lifecourse in the general population: a systematic review. BMC Psychiatry 9, 31 (2009).
-
Ram, N. & Grimm, K. J. Methods and measures: growth mixture modeling: a method for identifying differences in longitudinal change among unobserved groups. Int. J. Behav. Dev. 33, 565–576 (2009).
-
Balsamo, M., Cataldi, F., Carlucci, L. & Fairfield, B. Assessment of anxiety in older adults: a review of self-report measures. Clin. Interv. Aging https://doi.org/10.2147/CIA.S114100 (2018).
-
Spitzer, R. L., Kroenke, K., Williams, J. B. W. & Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166, 1092 (2006).
-
Sapra, A., Bhandari, P., Sharma, S., Chanpura, T. & Lopp, L. Using Generalized Anxiety Disorder-2 (GAD-2) and GAD-7 in a primary care setting. Cureus https://doi.org/10.7759/cureus.8224 (2020).
-
Holmes, S. E. et al. Trajectories of depressive and anxiety symptoms in older adults: a 6-year prospective cohort study. Int. J. Geriatr. Psychiatry 33, 405–413 (2018).
-
Cheng, Y., Thorpe, L., Kabir, R. & Lim, H. J. Latent class growth modeling of depression and anxiety in older adults: an 8-year follow-up of a population-based study. BMC Geriatr. 21, 550 (2021).
-
Kessler, R. C. et al. Mild disorders should not be eliminated from the DSM-V. Arch. Gen. Psychiatry 60, 1117 (2003).
-
Russell, A. et al. Protocol for a feasibility study and randomised pilot trial of a low-intensity psychological intervention for depression in adults with autism: the Autism Depression Trial (ADEPT). BMJ Open 7, e019545 (2017).
-
Quinton, A. M. G., Ali, D., Danese, A., Happé, F. & Rumball, F. The assessment and treatment of post-traumatic stress disorder in autistic people: a systematic review. Rev. J. Autism. Dev. Disord. https://doi.org/10.1007/s40489-024-00430-9 (2024).
-
McAdams, E., Quinton, A. M. G., Charlton, R., Happé, F. & Stewart G. R. Trauma and PTSD symptoms: exploring the experiences of autistic and non-autistic adults in midlife and old age. Preprint at Research Square https://doi.org/10.21203/rs.3.rs-7799328/v1 (2025).
-
Mansour, H. et al. Prevalence of post-traumatic stress disorder (PTSD) in autistic children or young people (CYP) and adults: a systematic review and meta-analysis. Clin. Psychol. Rev. 120, 102621 (2025).
-
Mason, D. et al. A systematic review of what barriers and facilitators prevent and enable physical healthcare services access for autistic adults. J. Autism. Dev. Disord. 49, 3387–3400 (2019).
-
Mansour, H. et al. ‘It’s designed for someone who is not me’: a reflexive thematic analysis of the unmet healthcare support needs in UK autistic adults aged 65 years and over. Autism 29, 754–765 (2025).
-
Viner, H. E., Yuill, N., Costa, A. P., Radford, H. & Kornadt, A. E. A qualitative interview study on quality of life and ageing experiences of autistic adults. Commun. Psychol. 2, 99 (2024).
-
Francis, D., Hershman, D., Charlton, R. A., Happé, F. & Stewart, G. R. “Bigger lows, but higher highs”: a qualitative exploration of the similarities and differences in quality of life of middle-aged and older autistic and non-autistic adults. Research in Autism 123, 202533 (2025).
-
Conner, K. O. et al. Mental health treatment seeking among older adults with depression: the impact of stigma and race. Am. J. Geriatr. Psychiatry 18, 531–543 (2010).
-
Curran, P. J. & Muthén, B. O. The application of latent curve analysis to testing developmental theories in intervention research. Am. J. Community Psychol. 27, 567–595 (1999).
-
Fischer, E. H., Dornelas, E. A. & Goethe, J. W. Characteristics of people lost to attrition in psychiatric follow-up studies. J. Nerv. Ment. Dis. 189, 49–55 (2001).
-
Putnam, O. C., Eddy, G., Crowley LaPoint, S., Swisher, M. & Harrop, C. “I’m excited to have my voice heard”: understanding autism research participation from the perspective of autistic women, non-binary adults, and parents of autistic girls. Neurodiversity 3, 27546330251324007 (2025).
-
Golomb, B. A. et al. The older the better: are elderly study participants more non-representative? A cross-sectional analysis of clinical trial and observational study samples. BMJ Open 2, e000833 (2012).
-
Farhane-Medina, N. Z., Luque, B., Tabernero, C. & Castillo-Mayén, R. Factors associated with gender and sex differences in anxiety prevalence and comorbidity: a systematic review. Sci. Prog. 105, 00368504221135469 (2022).
-
Allison, C., Auyeung, B. & Baron-Cohen, S. Toward brief “red flags” for autism screening: the short autism spectrum quotient and the short quantitative checklist in 1,000 cases and 3,000 controls. J. Am. Acad. Child Adolesc. Psychiatry 51, 202–212 (2012).
-
Eriksson, J. M., Andersen, L. M. & Bejerot, S. RAADS-14 Screen: validity of a screening tool for autism spectrum disorder in an adult psychiatric population. Mol. Autism. 4, 49 (2013).
-
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613 (2001).
-
Muthén, L. K. & Muthén, B. O. Mplus User’s Guide Eighth edn (Muthén & Muthén, 2017); https://www.statmodel.com/download/usersguide/MplusUserGuideVer_8.pdf
-
Stata Statistical Software (Stata Corp, 2017).
Acknowledgements
We thank the middle-aged and older autistic people who were involved in our research as steering group members. In their renumerated roles, they provided lived experience insights that informed the direction of this manuscript. The current study was not preregistered.
Funding
This research was funded by the Dunhill Medical Trust (now Vivensa Foundation), the British Academy, the National Institute for Health and Care Research (NIHR), the NIHR Biomedical Research Centre at South London, the NIHR Collaboration for Leadership in Applied Health Research and Care South West Peninsula, and the NIHR Exeter Clinical Research Facility. The funders have had no role in the data collection, analysis, interpretation or any other aspect pertinent to the study. The authors have not been paid to write this Article by any agency. This Article represents independent research conducted by the authors, and the views expressed are those of the author(s) and not necessarily those of the funders.
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Mental Health thanks Lauren Baczewski, Carolien Torenvliet and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eshetu, A., Ghai, S., Corbett, A. et al. The association between autistic traits and trajectories of anxiety in middle-aged and older adults: an 8-year growth mixture model analysis. Nat. Mental Health (2026). https://doi.org/10.1038/s44220-026-00654-0
-
Received:
-
Accepted:
-
Published:
-
Version of record:
-
DOI: https://doi.org/10.1038/s44220-026-00654-0
Leave a Reply