⏱ 8 min read
A 2026 medRxiv study of 30 adults with drug-resistant focal epilepsy found that dynamic FDG-PET had higher model-adjusted signal quality than static PET in most brain regions, including >80% posterior probability of superiority in 29 of 36 regions.
Research Highlights
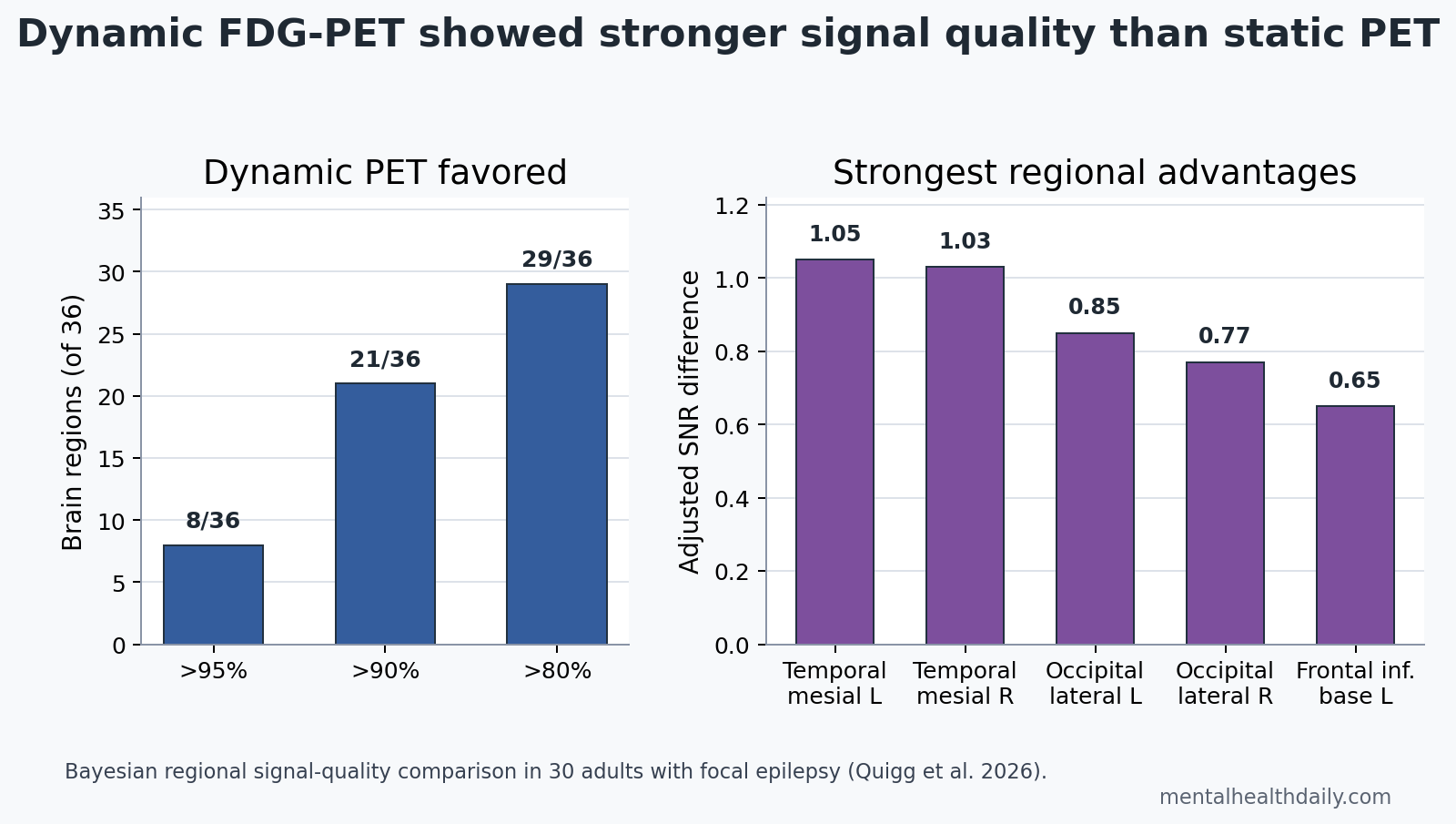
- Dynamic PET beat static PET: interictal dynamic FDG-PET showed higher signal quality than static PET with >95% probability in 8 of 36 regions, >90% probability in 21 regions, and >80% probability in 29 regions.
- Temporal regions led the result: left and right mesial temporal regions had the largest adjusted signal-to-noise advantages, with posterior medians of 1.05 and 1.03.
- Static PET rarely had the edge: only 5 regions favored static PET, and those probabilities ranged from 51% to 76%, which is not a strong static-PET signal.
- The method is not yet a clinical outcome test: the 30-person study compared signal quality, not seizure-freedom prediction, diagnostic sensitivity, or surgical decision changes.
- Temporal lobe epilepsy may be the target use case: mesial temporal regions had the top posterior medians, 1.05 on the left and 1.03 on the right.
Dynamic FDG-PET measures how quickly the brain takes up 18F-fluorodeoxyglucose, a radioactive glucose-like tracer used to map brain metabolism. Standard static FDG-PET usually measures tracer concentration after a waiting period, so it gives a late snapshot rather than a kinetic curve.
That distinction matters in focal epilepsy because an epileptogenic zone can be metabolically abnormal without having an obvious structural lesion. A static tracer snapshot may look normal when the rate of glucose uptake is the cleaner signal.
Dynamic FDG-PET Had Higher Signal Quality in 29 of 36 Regions
Quigg et al. analyzed adults with drug-resistant focal epilepsy who had dynamic FDG-PET, static PET maps extracted from the same acquisition, and MRI coregistration. Of 32 enrolled and scanned patients, 30 were usable for analysis; 2 were excluded because of tracer quality or missing MRI data for coregistration.
Signal-to-noise ratio compares useful signal with background variability. A higher value means the imaging map carries a stronger regional signal relative to noise, but it does not automatically mean the image correctly localizes the seizure-onset zone.
The researchers used Bayesian regional estimated signal quality (BRESQ), a hierarchical model that adjusted for patient differences, brain-region size, region location, and spatial correlation between regions. Instead of p-values, the model reported posterior probability that dynamic PET had better signal quality than static PET in each region.
The headline pattern was broad dynamic-PET superiority:
- >95% probability: dynamic PET was superior in 8 of 36 regions.
- >90% probability: dynamic PET was superior in 21 of 36 regions.
- >80% probability: dynamic PET was superior in 29 of 36 regions.
- Static-PET-favoring regions: 5 regions favored static PET, but only weakly, with posterior probabilities from 51% to 76%.
The best reading is not that static PET is obsolete. It is that dynamic PET produced cleaner modeled regional signal in this 30-person focal epilepsy cohort, which makes it worth testing against clinical localization outcomes.
Mesial Temporal Cortex Showed the Strongest Dynamic-PET Advantage
The largest adjusted signal-quality differences appeared in the left and right mesial temporal regions. The left mesial temporal region had a posterior median difference of 1.05, a 95% credible interval of 0.35 to 1.65, and 99.51% probability favoring dynamic PET. The right mesial temporal region was similar: posterior median 1.03, 95% credible interval 0.32 to 1.67, and 99.32% probability favoring dynamic PET.
Credible interval is the Bayesian interval that contains the model parameter with a specified probability, given the data and model. A 95% credible interval that stays above zero supports a positive dynamic-PET advantage in that region.
Other top regions included the left and right lateral occipital regions and the left frontal inferior base. The broader pattern looked ventral-to-dorsal rather than evenly distributed across the cortex.
That regional pattern is clinically interesting because temporal lobe epilepsy is one of the main presurgical localization problems where noninvasive imaging matters. If dynamic PET gains the most signal in mesial temporal regions, the most realistic next test is not a generic brain-mapping claim; it is whether dynamic PET improves lateralization or localization in temporal lobe epilepsy when MRI or static PET is ambiguous.
Static PET Has Known Blind Spots in Epilepsy Surgery Workups
Static FDG-PET is already part of presurgical epilepsy evaluation, especially when MRI does not show a clear lesion. It can reveal interictal hypometabolism, meaning lower metabolism between seizures in tissue involved in the epileptic network.
The limitation is that static PET does not always show a focal abnormality. Quigg et al. cited a large multicenter presurgical epilepsy study in which static PET was normal in 48% of surgical-candidate cases. A normal static PET does not prove absence of a metabolic epileptic zone; it may mean the static snapshot lacks enough contrast for that patient or region.
Earlier dynamic-PET work from the same research group gives the new signal-quality analysis its rationale. Seshadri et al. reported a pilot study of dynamic FDG-PET for focal epilepsy localization, including patients whose static PET did not show a lesion. Quigg and Kundu later described dynamic FDG-PET as a way to demonstrate functional brain abnormalities by modeling tracer uptake rates rather than only tracer concentration.
Metabolic-rate mapping is the key conceptual shift. Static PET asks where the tracer ended up after uptake. Dynamic PET asks how the uptake process unfolded over time. In focal epilepsy, that kinetic information may pick up altered neuronal activity, connectivity, or mitochondrial energy handling that a late static image compresses into a less specific signal.
Signal Quality Is Not the Same as Surgical Localization Accuracy
Evidence-strength note: this was a single-center, 30-person, methods-focused preprint that had not been certified by peer review. It supports the idea that dynamic FDG-PET can produce stronger regional signal than static PET. It does not prove that dynamic PET improves epilepsy surgery outcomes.
The next evidence step needs a different endpoint. Useful clinical validation would compare dynamic-PET abnormalities against seizure-onset-zone localization, intracranial EEG when available, surgical resection margins, and seizure freedom after surgery. A signal-quality advantage is necessary for a better map, but it is not sufficient.
Several design limits keep the result calibrated:
- Derived static comparator: static PET was extracted from the dynamic acquisition, which improves within-patient comparison but differs from a separate clinical static PET session.
- Broad regions: the model used 36 regions of interest, which is useful for signal-quality ranking but coarser than surgical targeting.
- Adult focal epilepsy sample: the result does not automatically apply to pediatric epilepsy, generalized epilepsy, or nonepileptic events.
- No outcome anchor: the paper did not report sensitivity, specificity, or seizure-freedom prediction.
Those limits do not erase the signal. They define the correct claim: dynamic FDG-PET looks technically stronger than static PET in many focal epilepsy regions, especially mesial temporal cortex, but clinical utility still has to be proven against patient-level decisions.
Why Dynamic PET Might Help When Static PET Looks Normal
One biological explanation is that epilepsy-related metabolic impairment is partly kinetic. FDG behaves like glucose, and brain uptake reflects both synaptic activity and energy metabolism. If the abnormal tissue differs more in uptake rate than in final tracer concentration, a static image can understate the abnormality.
Mechanistic epilepsy literature supports metabolic signal as real biology. Tenney et al. linked cerebral glucose hypometabolism with mitochondrial dysfunction in intractable epilepsy and cortical dysplasia, while older work connected hippocampal glucose oxidation capacity with interictal FDG-PET in temporal lobe epilepsy.
Normal regional metabolism also varies. Quigg et al. noted that a database of healthy adult static FDG-PET images found relatively low activity in temporal regions, including mesial and neocortical temporal cortex. A lower static background may make kinetic mapping more useful in regions where static tracer concentration is already difficult to interpret.
Clinical implication: dynamic PET is most promising where static PET is most likely to be inconclusive but localization still matters. That puts MRI-negative or static-PET-negative temporal lobe epilepsy near the front of the queue for validation, not because the current study proved outcome benefit, but because the regional signal pattern points there.
Questions About Dynamic FDG-PET in Focal Epilepsy
Is dynamic FDG-PET ready to replace static PET?
No. The 2026 preprint showed higher signal quality in most modeled regions, but it did not test whether dynamic PET changed surgical decisions or predicted seizure freedom better than static PET.
What does dynamic PET measure that static PET misses?
Dynamic PET measures tracer uptake kinetics over a 60-minute scan. Static PET measures tracer concentration during a later, shorter acquisition window. Kinetic mapping may reveal rate-of-uptake abnormalities that a late concentration image blurs.
Why were temporal regions important?
Left and right mesial temporal regions had the strongest dynamic-PET signal-quality advantages. That matters because temporal lobe epilepsy is a common presurgical localization problem and static PET can be normal or ambiguous in some candidates.
What would prove clinical utility?
A prospective study would need to show that dynamic FDG-PET improves seizure-onset-zone localization, changes management appropriately, and predicts seizure freedom after surgery beyond MRI, EEG, static PET, and other standard presurgical data.
References
- Quigg M, Chernyavskiy P, Terrell W, Smetana R, Muttikal TE, Wardius M, et al. Signal-to-noise evaluation of dynamic versus static 18FDG-PET in focal epilepsy via Bayesian regional estimated signal quality analysis. medRxiv. 2026. doi:10.64898/2026.04.12.26350712
- Steinbrenner M, Duncan JS, Dickson J, et al. Utility of 18F-fluorodeoxyglucose positron emission tomography in presurgical evaluation of patients with epilepsy: A multicenter study. Epilepsia. 2022. PubMed
- Seshadri V, Zarroli KA, Schetlick RS, et al. Dynamic FDG-PET in localization of focal epilepsy: A pilot study. Epilepsy & Behavior. 2021;122:108204. doi:10.1016/j.yebeh.2021.108204
- Quigg M, Kundu BK. Dynamic FDG-PET demonstration of functional brain abnormalities. Annals of Clinical and Translational Neurology. 2022;9:1487-1497. PubMed
- Tenney JR, Rozhkov L, Horn P, et al. Cerebral glucose hypometabolism is associated with mitochondrial dysfunction in patients with intractable epilepsy and cortical dysplasia. Epilepsia. 2014;55:1415-1422. PubMed
- Merida I, Jung J, Bouvard S, et al. CERMEP-IDB-MRXFDG: a database of 37 normal adult human brain FDG-PET, T1 and FLAIR MRI, and CT images available for research. EJNMMI Research. 2021;11:91. PubMed
Leave a Reply