Main
Childhood maltreatment is a key modifiable risk factor for poor mental health1. Childhood maltreatment can be measured through either prospective measures, typically derived from informant reports and observations, or retrospective self-reported measures, which identify largely non-overlapping groups2. Nevertheless, much of our understanding of its long-term effects and underlying mechanisms comes from studies comparing groups of individuals with versus without retrospective self-reports of maltreatment, which are quicker, easier and cheaper to collect than prospective measures3. Retrospective self-reports also show stronger associations with psychopathology than prospective measures, regardless of whether they are corroborated by prospective evidence4,5. But how stable is this method of classification over time?
Instability in childhood maltreatment reports could pose serious threats to both research and practice. Concerns about the low temporal stability of retrospective self-reports stem from their reliance on memory and subjective interpretation, which can be influenced by cognitive biases, emotional states and reappraisals over time3,6,7,8,9. Furthermore, the instability of childhood maltreatment reports may be compounded by normative developmental changes in autobiographical memory10,11,12. From a neurobiological perspective10,13, early life memories depend heavily on an immature hippocampal system, resulting in weaker encoding and inefficient consolidation—a combination that contributes to rapid forgetting and childhood amnesia. In contrast, with age, the hippocampus matures, supporting stronger episodic encoding, and hippocampal–cortical connectivity increases substantially. These expanding connections with distributed cortical networks (supported by schema-based organization and repeated retrieval or narrative rehearsal) enhance systems consolidation and may lead to greater long-term retention and reduced forgetting in later life. Low stability of retrospective maltreatment measures contributes to measurement error and misclassification14. In turn, misclassification could lead researchers to underestimate associations between maltreatment and outcomes, observe inconsistent findings across studies and struggle to identify underlying mechanisms by weakening mediation and moderation tests. Similarly, misclassification could lead legal, social care and clinical practitioners to provide inadequate or inappropriate interventions to mitigate the impact of childhood maltreatment.
Several studies15,16 have empirically tested the stability of retrospective self-reports with inconsistent results, highlighting the need for a quantitative summary and a better understanding of the heterogeneity in the literature. Several factors may explain the inconsistencies. First, the maltreatment type (for example, abuse versus neglect) may be relevant, as experiences can differ in their emotional salience and thus be differentially appraised and recalled over time17. Second, the sample characteristics: convenience samples may show higher stability than population-representative samples because of the effects of self-selection18,19 or differential attrition over time20; clinical samples are a pertinent example, in which participants with psychiatric diagnoses may show higher stability of recall than healthy controls due to cognitive mechanisms linked to psychopathology (for example, mood congruency effects, rumination, causal search biases or increased reflection on the past in therapy)21,22,23. Third, measurement type (for example, interviews versus questionnaires), as interviews may reduce measurement error by allowing clarifications but are also more prone to social desirability bias7,24, whereas questionnaires may be more prone to measurement error but offer privacy that may enhance consistency25. Fourth, demographic factors: some evidence suggests that female individuals may show higher report stability than male individuals16; younger age may also be associated with lower stability, as children and adolescents may initially struggle to identify maltreatment, have less developed memory processes and continue developing their identity and life narratives12,26,27,28. Fifth, the follow-up interval may be a factor, as longer intervals could be associated with lower stability, consistent with the forgetting curve29,30.
Results
Search results
The systematic search identified 49 studies examining the stability of self-reports of child maltreatment15,16,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77 (Table 1 and Supplementary Fig. 2). The studies were based on 49 cohorts (although 1 study used 2 different cohorts, and 1 cohort was used by 2 studies). There were 92,807 individuals assessed at baseline and 38,332 of these individuals were retained at follow-up, with an average attrition rate of 59%. Participants were 60.4% female, the average age at baseline assessment was 32.2 years (range = 13.2–68.5, median = 33.0), the average age at follow-up assessment was 34.4 years and the average follow-up interval was 2.4 years (123.6 weeks; range = 2 months to 12 years). The study quality assessment is described in Supplementary Table 1.
Stability of self-reports of maltreatment
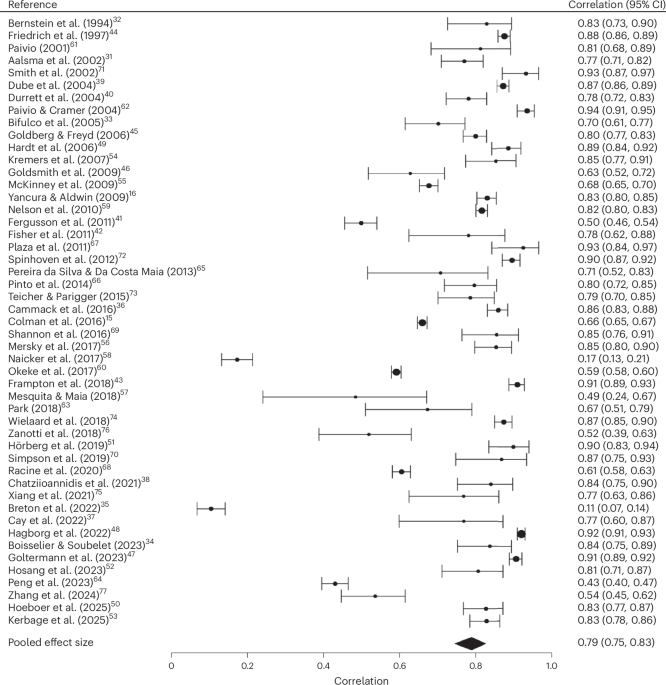
The overall meta-analytic estimate for the stability of self-reports of childhood maltreatment based on 235 effect sizes was r = 0.79 (95% confidence interval (CI), 0.75, 0.83), with heterogeneity I2 = 98.69 (Fig. 1). When excluding the 34 effect sizes from 11 studies estimated from the calibration model, the meta-analytic findings were very similar (r = 0.79; 95% CI, 0.74, 0.83).
The overall pooled effect size was 0.79. Points represent the correlation estimate for each study and horizontal error bars represent the corresponding 95% confidence intervals. For clarity of presentation, the forest plot shows a single effect size per study (reflecting the mean of all individual effect sizes obtained from each study). The mean effect size per study and its variance were calculated using the MAd package in R (R Foundation). Data from refs. 15,16,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77.
The results were not biased by small study effects (that is, publication bias) (P = 0.561) (Supplementary Fig. 3). The results were also not biased by undue effects of individual effect sizes (estimates from leave-one-out analyses ranged between 0.788 and 0.793), individual studies (range = 0.785–0.800; Supplementary Fig. 4) or individual cohorts (range = 0.785–0.800; Supplementary Fig. 5).
To illustrate the overall stability estimate, we also computed the approximate proportion of participants changing their responses between time points, based on the observed prevalence rates and correlation from population-representative studies. This indicated that approximately 20% of participants changed their responses, with 11% shifting from reporting maltreatment at baseline to not reporting it at follow-up and 9% shifting from not reporting maltreatment at baseline to reporting it at follow-up (Fig. 2).
Prevalence rates at baseline and follow-up were derived from k = 5 population-representative studies15,35,44,58,60 reporting 2 × 2 contingency tables. We extracted the proportion of participants reporting maltreatment at each time point, averaging 41% at time 1 and 39% at time 2. Using these prevalence estimates and a correlation of r = 0.79, we iteratively searched for the combination of response shifts that produced the observed change in prevalence and best approximated the target correlation. This yielded an estimate of approximately 20% of participants changing their response: 11% shifting from reporting maltreatment at baseline to not reporting it at follow-up, and 9% newly reporting maltreatment at follow-up despite not endorsing it at baseline.
Predictors of heterogeneity in the stability of self-reports of maltreatment
We next examined various possible sources of the high heterogeneity in the stability estimate (Table 2).
Stability was moderated by the maltreatment type (Q for moderation = 25.83; P < 0.0001), with lower stability estimates for physical neglect relative to physical abuse, sexual abuse, emotional abuse, maltreatment and adverse childhood experiences (ACEs), and lower stability estimates for emotional neglect relative to physical abuse and sexual abuse. In a post hoc analysis, we also found that stability estimates were significantly lower for overall measures of neglect (number of studies (k) = 25; r = 0.72; 95%CI, 0.65, 0.78) than abuse (k = 45; r = 0.81; 95% CI, 0.76, 0.84; Q for moderation = 19.94; P < 0.0001).
Stability was also moderated by the type of sample used (Q for moderation = 11.54; P = 0.003), with population-representative samples showing significantly lower stability estimates compared with non-representative convenience samples or clinical samples. The overall meta-analytic estimate was not moderated by the assessment method (interview versus questionnaire). Furthermore, a post hoc analysis of studies using questionnaires showed a non-significant difference in stability estimates between those with single-item measures (k = 6; r = 0.73; 95% CI, 0.61, 0.82) and those with multi-item measures (k = 37; r = 0.81; 95% CI, 0.60, 0.92; Q for moderation = 3.03; P = 0.08).
Baseline and follow-up age moderated the effect size estimate, with stability increasing with age (baseline age, Q for moderation = 7.02, P = 0.008; follow-up age, Q for moderation = 4.59, P = 0.032). Visual inspection (Supplementary Fig. 6) indicated that the stability did not vary linearly with baseline age, with notably lower stability estimates among younger participants. The addition of a logarithmic term improved model fit compared with a linear model in the meta-regression (likelihood ratio test χ2 = 5.501, P = 0.019) (Supplementary Fig. 7). Furthermore, we found that studies with baseline ages between 0 and 18 years (k = 8; r = 0.65; 95% CI, 0.49, 0.77) had lower stability compared with studies with baseline ages greater than 18 years (k = 40; r = 0.81; 95% CI, 0.77, 0.85; Q for moderation = 6.88; P = 0.009). We also repeated this moderation analysis using alternative cut-off points to define childhood and adolescence, and observed a similar pattern of results when applying cut-offs at ages 21 and 24 (Supplementary Table 2).
Stability was not significantly moderated by time interval (Q for moderation = 2.96, P = 0.085) (Table 2). We further explored whether the associations between time interval and stability differed depending on baseline age. We found a significant interaction effect (unstandardized meta-regression coefficient (b) = 0.002; 95% CI, 0.0001, 0.005; P = 0.04), indicating that stability decreased over time for participants under 18, while it remained stable over time for adults (Supplementary Table 3). On the basis of predictions from this model, stability was r = 0.59 for those under 18 and r = 0.81 for adults at 2.5 years, and r = 0.31 and r = 0.79, respectively, at 5 years (Fig. 3). We repeated these analyses for the alternative age cut-offs for childhood and adolescence, and found a comparable pattern of results (Supplementary Figs. 8 and 9 and Supplementary Table 3).
Predictions from an interaction model between baseline age (age 18 cut-off) and follow-up interval, inverse-transformed to the correlation scale for 0–261 weeks (0–5 years), showing that stability decreased over time for participants under 18 but remained stable over time for adults. The lines represent the predicted correlation estimates from the interaction model for adults and participants under 18 across follow-up intervals, and the gray shaded areas represent the corresponding 95% confidence intervals around these predictions.
We considered that lower stability for participants under 18 might reflect new exposures rather than changes in self-reports over time. In a sensitivity analysis excluding 2 studies that included participants under 18 but did not explicitly specify the same reporting period across time points35,63, we found a similar meta-analytic estimate (r = 0.80; 95% CI, 0.76, 0.83). The moderation analyses focusing on baseline age and the interaction between baseline age and follow-up interval yielded a similar patterns of results, although the results did not reach statistical significance (P = 0.10 for the moderation model, P = 0.09 for the interaction model; Supplementary Fig. 10 and Supplementary Tables 4 and 5). However, when we repeated these analyses using the broader age cut-offs for childhood and adolescence, we observed significant moderation and interaction effects (Supplementary Figs. 11 and 12 and Supplementary Tables 4 and 5).
We also conducted a post hoc moderation analysis to examine whether stability estimates differed by effect size type. We found significant differences (Q for moderation = 14.1, P = 0.001), with greater stability in studies using intraclass correlation coefficients (ICCs) (k = 17; r = 0.86; 95% CI, 0.82, 0.89) than in those using tetrachoric (k = 24; r = 0.75; 95% CI, 0.69, 0.81) and Pearson’s or Spearman’s correlations (k = 10; r = 0.72; 95% CI, 0.59, 0.81).
The meta-analytic estimate was not significantly moderated by sex distribution, attrition rate or the study quality.
Within the subset of studies with clinical samples, stability was not moderated by the proportion of individuals with clinical diagnoses, the type of psychopathology or the presence of an intervention between baseline and follow-up (Table 3; see Supplementary Table 6 for a description of studies that included an intervention). Similar results were observed in sensitivity analyses restricted to studies that did not include healthy volunteers (Supplementary Table 7).
Discussion
This systematic review and meta-analysis of 49 studies including 38,332 individuals found that retrospective self-reports of childhood maltreatment were stable over an average follow-up period of 2.4 years. Despite the high stability of the reports, 1 in 5 (20%) participants changed their responses over the observational period (at follow-up, 11% omitted reports made at baseline and 9% provided new reports that were not made at baseline; Fig. 2). The overall meta-analytic effect size of r = 0.79 is consistent with the high long-term stability observed for the self-reports of broader measures of childhood experiences78 and the stability of key psychological constructs, such as cognition79. The overall meta-analytic estimate showed high heterogeneity and should therefore be interpreted with caution. To better understand this heterogeneity, we undertook moderation analyses, which identified factors that influence stability and important gaps in our current knowledge.
First, sample type moderated stability. Population-representative samples showed significantly lower stability than both non-representative convenience samples and clinical samples—differences that might emerge for several reasons. For example, measure characteristics might have differed across sample types: larger, population-representative samples may use briefer, less detailed assessments, increasing the likelihood of reporting inconsistency. However, we found limited support for this hypothesis. We did not find that the use of interviews versus questionnaires moderated stability estimates, and a post hoc analysis indicated that the difference in stability between studies using multi-item versus single-item questionnaires was not statistically significant (trend).
Participant characteristics may explain stability differences between sample types. Participants in population-representative samples, who do not self-select into research, may have less survey experience, weaker topic knowledge, lower certainty or lower introspection about their experiences, reducing report stability18. For example, in the UK Biobank study19, participants with lower participation probability made more self-report errors in supposedly time-invariant variables and errors increased after adjusting for participation bias, suggesting greater stability in non-representative samples.
Clinical samples also showed higher stability than population-representative samples, likely due to cognitive mechanisms linked to psychopathology. For example, the mood congruency model suggests that negative memories are more easily recalled in low mood states21,80, while rumination—common in depression, anxiety and post-traumatic stress disorder (PTSD)—may enhance recall over time through repeated rehearsal22. Greater reflection during treatment may further enhance memory accessibility. Causal search bias, where individuals reinterpret past experiences to explain their distress or difficulties, could also increase consistency by reinforcing negative interpretations of memories over time23. Finally, more severe or chronic maltreatment experiences may heighten both psychopathology risk and recall consistency over time17. Of note, stability did not vary by psychopathology type, suggesting that transdiagnostic rather than disorder-specific mechanisms may be driving higher stability in clinical populations.
Second, maltreatment type moderated stability. Reports of neglect showed lower stability than reports of abuse or broader measures of maltreatment. This aligns with previous evidence that retrospective reports of neglect also show lower agreement with prospective measures of neglect compared with other maltreatment types2, suggesting greater variability in retrospective recall may partly explain this pattern. On the one hand, threatening experiences, such as abuse, may be more strongly encoded in memory and persist unscathed17,81. On the other hand, neglect involves the absence of actions or resources, rather than the occurrence of more tangible events that typically serve to anchor memories82, and its definition might vary over time as individuals and societies change their interpretations of what constitutes a child’s ‘basic needs’ and adequate caregiving practices83.
Third, age moderated stability. Report stability was significantly lower among participants who were first asked to recall maltreatment in childhood than those who were first asked to recall it in adulthood. Furthermore, stability significantly decreased as a function of follow-up duration in participants who first recalled maltreatment in childhood but not in those who first recalled it in adulthood. These findings should be interpreted with caution, as a sensitivity analysis excluding 2 studies involving under-18 participants, where new experiences might have affected reporting, showed similar patterns but weaker evidence. However, significant moderation and interaction effects were observed when using broader age cut-offs to define childhood and adolescence versus adulthood, even after excluding these 2 studies, suggesting that the non-significant finding at age 18 may reflect limited statistical power due to the smaller number of studies in this subgroup. The consistent effects across broader age definitions support the interpretation that younger participants show less stable reporting, particularly over longer periods.
These findings are consistent with a large body of literature11,12,26,27,84,85 on the developmental progression of autobiographical memory and life narratives, which become increasingly stable and coherent from childhood into adulthood thanks to social–cognitive development involving temporal sequencing, causal and thematic coherence, and the cultural concept of biography. Children’s and adolescents’ memories may be more malleable and susceptible to reinterpretation because of new knowledge, evolving life narratives and sense of self, and shifting social contexts26,28. In contrast, adults’ memories may be more stable over time because of repeated rehearsal and integration into a coherent life narrative27,85. Of note, similar patterns of moderation by age are also observed for highly stable traits, such as cognitive abilities and personality79,86, reflecting greater overall malleability of psychological processes in childhood and adolescence.
The findings should be interpreted in the context of some limitations. First, the number of population-representative samples was small, limiting the generalizability of the findings. Nevertheless, stability was relatively high (r = 0.62) even among population-representative samples. The findings should also be interpreted within the context of research studies similar to those included in the meta-analyses and may not generalize to other contexts (for example, to disclosures that reach the attention of authorities). Specifically, the included studies relied on research interviews or questionnaires completed in confidential research settings, which may elicit different reporting patterns than official or forensic disclosures made in the context of police interviews, investigations by child protection services or legal proceedings, where additional motivational factors may influence reporting.
Second, attrition rates were high, with an average loss of more than half the participants between baseline and follow-up. While no significant effect was detected in our moderation analysis, attrition could still introduce bias20, particularly because studies did not consistently report whether participants lost at follow-up systematically differed from those retained. For example, we found that stability is greatest in individuals with mental health problems (clinical samples), and greater attrition among individuals with mental health problems might reduce stability estimates in population samples.
Third, the average follow-up interval was 2.4 years—a relatively short time frame in which memories for major childhood events may be less likely to change. It will be important to test how stability varies over longer intervals, particularly in light of findings that even highly stable traits, such as personality, show greater decline in stability over longer intervals86.
Fourth, the number of studies with participants under 18 was limited, and in 2 studies35,63 it was unclear whether changes reflected shifts in self-reports over time or the occurrence of new experiences between assessments. Further research is needed to examine the stability of self-reports in children and adolescents, with a focus on ensuring consistency in the reporting period across assessments.
Fifth, the preregistered search strategy did not include databases from adjacent fields such as nursing, social work, education or criminology, where other relevant studies on maltreatment and trauma assessment might also be found. Moreover, it focused on core maltreatment terms and may have missed studies using broader descriptors such as violence or victimization. Future reviews could expand searches to include these terms and interdisciplinary databases to ensure more comprehensive coverage.
Sixth, we found differences in estimates by effect size type, ICC estimates showing significantly higher stability compared with tetrachoric or Pearson and Spearman correlations. However, although the differences are statistically significant, the effect sizes are qualitatively similar (all large) and support the same conclusion of high stability.
Finally, due to a lack of available data, we were unable to examine in detail the effects of several other factors on self-report stability, including event characteristics (for example, age at maltreatment occurrence, severity and duration), ethnicity, socioeconomic status, personality, cognitive abilities, changes in psychopathology15 or therapeutic intervention (only six studies included an intervention, only one of which was trauma-focused, that is, specifically targeting maladaptive cognitive appraisals or memory processes50) (Supplementary Table 6).
Our findings have important implications for research and practice. The high stability of retrospective maltreatment reports over an average of 2.4 years provides some reassurance about the relative stability of single time-point assessments of maltreatment in both research and applied settings, such as legal, social care and clinical contexts. This supports the use of retrospective measures as a stable feature, allowing researchers to categorize individuals as maltreated or non-maltreated with reasonable confidence, at least in the short term. It also suggests that the lack of agreement between prospective and retrospective measures is unlikely to be driven by shifting retrospective reports over time (that is, measurement error)14 and instead may be driven by stable individual differences in the way individuals do or do not recall maltreatment experiences2,7. More research is needed to better understand the developmental mechanisms underlying age-related differences in the stability of childhood maltreatment reports10,11,12,13.
There are nuanced implications for practice. The overall high stability of childhood maltreatment reports suggests that disclosures should be taken seriously and guide interventions in legal–forensic and social care settings. Nevertheless, a 20% change in reports highlights that professionals should anticipate some differences in reporting over time, particularly in children. In such cases, it is important to avoid premature conclusions about fabrication. Differences in reporting can reflect multiple processes, including changes in appraisal, the reconstructive nature of memory, changing motivational or contextual influences and errors7. This suggests that records of disclosure should include an account of the context and developmental factors. It also suggests the need to strengthen memory and developmental expertise among professionals working in this area. These implications for practice should be considered with caution, given the known research–practice gap: research and practice settings for reporting can be very different, and the greater stress, fear, stakes and lack of familiarity in practice settings might further influence report stability.
From a clinical perspective, our findings indicate that recall and cognitions surrounding maltreatment experiences are unlikely to change spontaneously over a few years, particularly in clinical populations. Retrospective recall of maltreatment is associated with heightened risk for subsequent psychiatric disorders, even accounting for previous history of psychopathology87. Therefore, the stability of maltreatment self-reports may help explain their association with chronicity and recurrence of emotional disorders88,89. Targeted interventions may be necessary to shift unhelpful appraisals and prevent or mitigate the lingering impact of maltreatment on psychopathology. Existing trauma-focused interventions (for example, trauma-focused cognitive behavioral therapy, eye movement desensitization and reprocessing, and imagery rescripting)90,91 already target maladaptive post-traumatic cognitions and memory processes in PTSD and might also be beneficial for the much broader set of trauma-related psychiatric disorders92. Because of the greater malleability of childhood maltreatment memories in childhood and adolescent years, such interventions may be more beneficial when delivered early in life. Children’s autobiographical memories are encoded with immature hippocampal systems and undergo inefficient consolidation, which may leave memories of early traumatic experiences comparatively unstable and modifiable. During childhood and adolescence—before these memories are fully integrated into cortical networks and narrative identity structures—therapeutic interventions could more easily influence how these memories are retrieved, elaborated and reconsolidated. As a result, trauma-focused treatments delivered early in life may have greater potential to shape how traumatic memories are ultimately organized and incorporated into the child’s developing autobiographical memory, thereby reducing long-term psychopathology.
Methods
Data sources
Following a predefined protocol registered on Prospero (identifier CRD42023414023), we conducted a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) and Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines (Supplementary Information). We searched Embase, PsycInfo and MEDLINE for peer-reviewed studies that measured the stability of self-reports of child maltreatment, were written in English and were published from database inception until 1 October 2025. Search terms were: (child* maltreatment, child* abuse, child* neglect, child* trauma, child* adver*, early life stress, adverse childhood experiences, ACEs) and (intrarater, test–retest, reliability, stability, reproducibility, consistency, repeatability, intraclass correlation coefficient, ICC, kappa).
Study selection
Titles and abstracts of all articles captured by the search were independently screened by one doctoral student (O.C.) and independent raters with undergraduate degree training who were blind to each other’s decisions (inter-rater agreement κ = 0.62). Full texts of potentially eligible studies were then screened independently following the same procedure (inter-rater agreement κ = 0.67). Inconsistencies were discussed and resolved with the senior author (A.D.). Peer-reviewed longitudinal studies with self-reports of child maltreatment assessed at least twice in the same individual participants were included. Deviating from the study’s pre-registration plan, we decided to include only studies with a time interval of 2 months or longer. This decision was guided by our interest in examining the stability of maltreatment memories over time rather than the short-term test–retest reliability of maltreatment measures; this resulted in the exclusion of k = 56 studies assessing the psychometric properties of maltreatment measures being developed.
Child maltreatment was defined as any of the following experiences between birth and age 18 years: physical abuse, sexual abuse, emotional abuse, physical neglect, emotional neglect, institutional neglect or deprivation, harsh physical discipline or corporal punishment, or broader measures of adversity that included any of the above forms of maltreatment.
Data extraction
Data were extracted independently by one doctoral student (O.C.) and double entered by an independent rater. Inconsistencies were discussed and resolved in consensus meetings. Data extraction included stability estimate(s), exposure type(s), sample characteristics (population representative, convenience or clinical sampling), measure type (interview versus questionnaire), demographic factors (sex and age at baseline and follow-up assessment), time interval between assessments, attrition rate and study quality characteristics (population representativeness of the sample, attrition rate, whether the measures were validated and whether the study controlled for the effects of sociodemographic or clinical variables on the stability estimate). For clinical samples, we also extracted data on the type of psychopathology and the presence of an intervention between baseline and follow-up
For studies that measured stability at multiple time points, the longest time interval was selected by default. This was guided by our interest in examining memory-related processes, which are more likely to emerge and become more pronounced over longer periods. However, in cases where a shorter interval provided a greater number of effect sizes, the shorter interval was chosen.
Statistical analysis
All analyses were conducted in R using the metafor package.
Studies reported different types of stability effect sizes, including Pearson and Spearman correlation coefficients, ICCs and Cohen’s κ coefficients. We initially harmonized all stability effect sizes onto a correlational scale using a calibration model to estimate tetrachoric correlations from κ statistics when necessary (Supplementary Methods and Supplementary Fig. 1). We then used Fisher’s z-transformation for the correlation effect sizes to stabilize the variance and achieve an approximately normal distribution, allowing us to calculate the variance using the z-transformed effect sizes and corresponding sample sizes with the escalc function in R. For clarity in reporting, the meta-analytic results were then inverse z-transformed and presented as correlations.
We estimated the overall meta-analytic effect size for the stability of self-reports of childhood maltreatment using a multilevel model (including random-sampling variance, within-study variance and between-study variance) to account for the non-independence of the data, as many studies contributed multiple effect sizes, for example across maltreatment types or subgroups (such as patients versus controls or male versus female participants). We used the I2 statistic to measure heterogeneity in the meta-analytical estimate. We then conducted sensitivity analyses testing for publication bias (an extension of the Egger’s test for multilevel meta-analysis models) and undue influence of cohorts, studies or effect sizes (leave-one-out analyses). A sensitivity analysis was also conducted to assess whether excluding studies where tetrachoric correlations were estimated using the calibration model affected the overall meta-analytic estimate (k = 11, n = 34).
We used meta-regressions to test whether stability was moderated by a set of a priori-defined factors, including type of maltreatment, type of sample (population-representative samples, non-representative convenience samples and clinical samples), type of measure (questionnaire or interview), sex distribution, age at assessment (baseline and follow-up), time interval between assessments, percentage loss to attrition and study quality. We also conducted a post hoc moderation analysis examining whether stability was moderated by effect size type (ICC, Pearson or Spearman’s correlation, or tetrachoric correlation).
As autobiographical memory undergoes major developmental changes from adolescence to adulthood, we conducted post hoc analyses using a binary age variable distinguishing studies with a mean baseline age of 18 years or younger (childhood and adolescence) from those with a mean baseline age over 18 years (adulthood) and tested moderation effects. We also fitted an interaction model between baseline age and follow-up interval to examine whether the effects of age on reporting stability varied by follow-up length, as developmental processes affecting memory may become more pronounced over longer intervals12. To assess the sensitivity of these findings to how developmental periods are defined, we repeated the moderation and interaction analyses using alternative cut-offs at ages 21 and 24, reflecting broader definitions of adolescence and emerging adulthood proposed in developmental frameworks93. Finally, we tested whether any observed effects of age on stability could be explained by newly occurring experiences in participants under 18 by restricting the analyses to studies explicitly specifying the same reporting period across time points.
Finally, within the subset of studies using a clinical sample, we tested whether the type of psychopathology moderated the effect size estimates and whether the presence of an intervention between baseline and follow-up influenced the association. To assess whether healthy volunteers influenced stability estimates in clinical studies, we also conducted a sensitivity analysis restricting sampling to studies that did not include healthy volunteers.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data extraction table is available via Code Ocean at https://doi.org/10.24433/CO.8392361.v1.
Code availability
The script for the analysis is available via Code Ocean at https://doi.org/10.24433/CO.8392361.v1.
References
-
Arango, C. et al. Risk and protective factors for mental disorders beyond genetics: an evidence-based atlas. World Psychiatry 20, 417–436 (2021).
-
Baldwin, J. R., Reuben, A., Newbury, J. B. & Danese, A. Agreement between prospective and retrospective measures of childhood maltreatment: a systematic review and meta-analysis. JAMA Psychiatry 76, 584–593 (2019).
-
Danese, A. Annual research review: rethinking childhood trauma-new research directions for measurement, study design and analytical strategies. J. Child Psychol. Psychiatry 61, 236–250 (2020).
-
Baldwin, J. R., Coleman, O., Francis, E. R. & Danese, A. Prospective and retrospective measures of child maltreatment and their association with psychopathology: a systematic review and meta-analysis. JAMA Psychiatry 81, 769–781 (2024).
-
Danese, A. & Widom, C. S. Objective and subjective experiences of child maltreatment and their relationships with psychopathology. Nat. Hum. Behav. 4, 811–818 (2020).
-
Brewin, C. R., Andrews, B. & Gotlib, I. H. Psychopathology and early experience: a reappraisal of retrospective reports. Psychol. Bull. 113, 82–98 (1993).
-
Coleman, O. et al. Research review: why do prospective and retrospective measures of maltreatment differ? A narrative review. J. Child Psychol. Psychiatry 65, 1662–1677 (2024).
-
Hardt, J. & Rutter, M. Validity of adult retrospective reports of adverse childhood experiences: review of the evidence. J. Child Psychol. Psychiatry 45, 260–273 (2004).
-
Widom, C. S., Raphael, K. G. & DuMont, K. A. The case for prospective longitudinal studies in child maltreatment research: commentary on Dube, Williamson, Thompson, Felitti, and Anda (2004). Child Abuse Negl. 28, 715–722 (2004).
-
Bauer, P. J. Development of episodic and autobiographical memory: the importance of remembering forgetting. Dev. Rev. 38, 146–166 (2015).
-
Habermas, T. & Bluck, S. Getting a life: the emergence of the life story in adolescence. Psychol. Bull. 126, 748–769 (2000).
-
Fivush, R. The development of autobiographical memory. Annu. Rev. Psychol. 62, 559–582 (2011).
-
Squire, L. R., Genzel, L., Wixted, J. T. & Morris, R. G. Memory consolidation. Cold Spring Harb. Perspect. Biol. 7, a021766 (2015).
-
Anastasi, A. & Urbina, S. Psychological Testing (Prentice Hall, 1997).
-
Colman, I. et al. Consistency in adult reporting of adverse childhood experiences. Psychol. Med. 46, 543–549 (2016).
-
Yancura, L. A. & Aldwin, C. M. Stability and change in retrospective reports of childhood experiences over a 5-year period: findings from the Davis Longitudinal Study. Psychol. Aging 24, 715–721 (2009).
-
Kensinger, E. A. & Schacter, D. L. in Handbook of Emotions (eds Lewis, M. et al.) 601–617 (The Guilford Press, 2008).
-
Chang, L. & Krosnick, J. A. National surveys via RDD telephone interviewing versus the internet. Public Opin. Q. 73, 641–678 (2009).
-
Schoeler, T., Pingault, J.-B. & Kutalik, Z. The impact of self-report inaccuracy in the UK Biobank and its interplay with selective participation. Nat. Hum. Behav. 9, 584–594 (2024).
-
Tyrrell, J. et al. Genetic predictors of participation in optional components of UK Biobank. Nat. Commun. 12, 886 (2021).
-
Blaney, P. H. Affect and memory: a review. Psychol. Bull. 99, 229–246 (1986).
-
Lyubomirsky, S., Caldwell, N. D. & Nolen-Hoeksema, S. Effects of ruminative and distracting responses to depressed mood on retrieval of autobiographical memories. J. Pers. Soc. Psychol. 75, 166–177 (1998).
-
Susser, E. & Widom, C. S. Still searching for lost truths about the bitter sorrows of childhood. Schizophr. Bull. 38, 672–675 (2012).
-
Conrad, F. G. & Schober, M. F. Clarifying question meaning in a household telephone survey. Public Opin. Q. 64, 1–28 (2000).
-
Kim, J., Dubowitz, H., Hudson-Martin, E. & Lane, W. Comparison of 3 data collection methods for gathering sensitive and less sensitive information. Ambul. Pediatr. 8, 255–260 (2008).
-
Köber, C. & Habermas, T. How stable is the personal past? Stability of most important autobiographical memories and life narratives across eight years in a life span sample. J. Pers. Soc. Psychol. 113, 608–626 (2017).
-
McLean, K. C. Stories of the young and the old: personal continuity and narrative identity. Dev. Psychol. 44, 254–264 (2008).
-
Stige, S. H., Halvorsen, J. E. & Solberg, E. T. Pathways to understanding—how adult survivors of child sexual abuse came to understand that they had been sexually abused. J. Child Sex. Abuse 29, 205–221 (2020).
-
Hardt, O., Nader, K. & Nadel, L. Decay happens: the role of active forgetting in memory. Trends Cogn. Sci. 17, 111–120 (2013).
-
Murre, J. M. J. & Dros, J. Replication and analysis of Ebbinghaus’ forgetting curve. PLoS ONE 10, e0120644 (2015).
-
Aalsma, M. C., Zimet, G. D., Fortenberry, J. D., Blythe, M. & Orr, D. P. Reports of childhood sexual abuse by adolescents and young adults: stability over time. J. Sex Res. 39, 259–263 (2002).
-
Bernstein, D. P. et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatry 151, 1132–1136 (1994).
-
Bifulco, A., Bernazzani, O., Moran, P. M. & Jacobs, C. The Childhood Experience of Care and Abuse Questionnaire (CECA.Q): validation in a community series. Br. J. Clin. Psychol. 44, 563–581 (2005).
-
Boisselier, N. & Soubelet, A. Measuring early life adversity in adults: French translation and validation of the Maltreatment and Abuse Chronology of Exposure (MACE) scale. Eur. J. Trauma Dissociation 7, 100336 (2023).
-
Breton, E., Kidman, R., Behrman, J., Mwera, J. & Kohler, H.-P. Longitudinal consistency of self-reports of adverse childhood experiences among adolescents in a low-income setting. SSM Popul. Health 19, 101205 (2022).
-
Cammack, A. L. et al. Test-retest reliability of retrospective self-reported maternal exposure to childhood abuse and neglect. Arch. Womens Ment. Health 19, 415–421 (2016).
-
Cay, M., Chouinard, V.-A., Hall, M.-H. & Shinn, A. K. Test-retest reliability of the Childhood Trauma Questionnaire in psychotic disorders. J. Psychiatr. Res. 156, 78–83 (2022).
-
Chatziioannidis, S., Agorastos, A., Kaprinis, S. & Bozikas, V.-P. Short-term reliability of retrospective childhood trauma reports in schizophrenia spectrum psychosis. Psychiatriki 32, 241–246 (2021).
-
Dube, S. R., Williamson, D. F., Thompson, T., Felitti, V. J. & Anda, R. F. Assessing the reliability of retrospective reports of adverse childhood experiences among adult HMO members attending a primary care clinic. Child Abuse Negl. 28, 729–737 (2004).
-
Durrett, C., Trull, T. J. & Silk, K. Retrospective measures of childhood abuse: concurrent validity and reliability in a nonclinical sample with borderline features. J. Personal. Disord. 18, 178–192 (2004).
-
Fergusson, D. M., Horwood, L. J. & Boden, J. M. Structural equation modeling of repeated retrospective reports of childhood maltreatment: modeling of reports of child maltreatment. Int. J. Methods Psychiatr. Res. 20, 93–104 (2011).
-
Fisher, H. L. et al. Reliability and comparability of psychosis patients’ retrospective reports of childhood abuse. Schizophr. Bull. 37, 546–553 (2011).
-
Frampton, N. M. A., Poole, J. C., Dobson, K. S. & Pusch, D. The effects of adult depression on the recollection of adverse childhood experiences. Child Abuse Negl. 86, 45–54 (2018).
-
Friedrich, W. N., Talley, N. J., Panser, L., Fett, S. & Zinmeister, A. R. Concordance of reports of childhood abuse by adults. Child Maltreat. 2, 164–171 (1997).
-
Goldberg, L. R. & Freyd, J. J. Self-reports of potentially traumatic experiences in an adult community sample: gender differences and test-retest stabilities of the items in a brief betrayal-trauma survey. J. Trauma Dissociation 7, 39–63 (2006).
-
Goldsmith, R. E., Freyd, J. J. & DePrince, A. P. To add insight to injury: childhood abuse, abuse perceptions, and the emotional and physical health of young adults. J. Aggress. Maltreatment Trauma 18, 350–366 (2009).
-
Goltermann, J. et al. Temporal stability and state-dependence of retrospective self-reports of childhood maltreatment in healthy and depressed adults. Psychol. Assess. 35, 12–22 (2023).
-
Hagborg, J. M., Kalin, T. & Gerdner, A. The Childhood Trauma Questionnaire–Short Form (CTQ-SF) used with adolescents—methodological report from clinical and community samples. J. Child Adolesc. Trauma 15, 1199–1213 (2022).
-
Hardt, J., Sidor, A., Bracko, M. & Egle, U. T. Reliability of retrospective assessments of childhood experiences in Germany. J. Nerv. Ment. Dis. 194, 676–683 (2006).
-
Hoeboer, C. M. et al. Validation of the Childhood Trauma Questionnaire (CTQ) in the context of trauma-focused treatment. Child Maltreat. https://doi.org/10.1177/10775595251328611 (2025).
-
Hörberg, N. et al. Early Trauma Inventory Self-Report Short Form (ETISR-SF): validation of the Swedish translation in clinical and non-clinical samples. Nord. J. Psychiatry 73, 81–89 (2019).
-
Hosang, G. M., Manoli, A., Shakoor, S., Fisher, H. L. & Parker, C. Reliability and convergent validity of retrospective reports of childhood maltreatment by individuals with bipolar disorder. Psychiatry Res. 321, 115105 (2023).
-
Kerbage, H. et al. Influence of depressive symptoms and current suicidality on the stability of responses to the childhood trauma questionnaire. Child Abuse Negl. 167, 107560 (2025).
-
Kremers, I. P., Van Giezen, A. E., Van Der Does, A. J. W., Van Dyck, R. & Spinhoven, P. Memory of childhood trauma before and after long-term psychological treatment of borderline personality disorder. J. Behav. Ther. Exp. Psychiatry 38, 1–10 (2007).
-
McKinney, C. M., Harris, T. R. & Caetano, R. Reliability of self-reported childhood physical abuse by adults and factors predictive of inconsistent reporting. Violence Vict. 24, 653–668 (2009).
-
Mersky, J. P., Janczewski, C. E. & Topitzes, J. Rethinking the measurement of adversity: moving toward second-generation research on adverse childhood experiences. Child Maltreat. 22, 58–68 (2017).
-
Mesquita, C. S. & Maia, ÂC. What is told when the story is retold? Consistency of victimization reports in psychiatric patients. Scand. J. Psychol. 59, 311–318 (2018).
-
Naicker, S. N., Norris, S. A., Mabaso, M. & Richter, L. M. An analysis of retrospective and repeat prospective reports of adverse childhood experiences from the South African Birth to Twenty Plus cohort. PLoS ONE 12, e0181522 (2017).
-
Nelson, E. C., Lynskey, M. T., Heath, A. C., Madden, P. A. F. & Martin, N. G. A family study of adult twins with and without a history of childhood abuse: stability of retrospective reports of maltreatment and associated family measures. Twin Res. Hum. Genet. 13, 121–130 (2010).
-
Okeke, N. L., Wilkinson, A. V. & Roberts, R. E. The stability of retrospective child sexual abuse reports and its association with problem avoidance. J. Child Sex. Abuse 26, 677–691 (2017).
-
Paivio, S. C. Stability of retrospective self-reports of child abuse and neglect before and after therapy for child abuse issues. Child Abuse Negl. 25, 1053–1068 (2001).
-
Paivio, S. C. & Cramer, K. M. Factor structure and reliability of the Childhood Trauma Questionnaire in a Canadian undergraduate student sample. Child Abuse Negl. 28, 889–904 (2004).
-
Park, S. Reliability and validity of the Early Trauma Inventory Self Report-Short Form among Korean adolescents. J. Korean Acad. Child Adolesc. Psychiatry 29, 2–6 (2018).
-
Peng, C., Cheng, J., Rong, F., Wang, Y. & Yu, Y. Psychometric properties and normative data of the childhood trauma questionnaire-short form in Chinese adolescents. Front. Psychol. 14, 1130683 (2023).
-
Pereira Da Silva, S. S. & Da Costa Maia, Â. The stability of self-reported adverse experiences in childhood: a longitudinal study on obesity. J. Interpers. Violence 28, 1989–2004 (2013).
-
Pinto, R., Correia, L. & Maia, Â. Assessing the reliability of retrospective reports of adverse childhood experiences among adolescents with documented childhood maltreatment. J. Fam. Violence 29, 431–438 (2014).
-
Plaza, A. et al. Validation and test-retest reliability of Early Trauma Inventory in Spanish postpartum women. J. Nerv. Ment. Dis. 199, 280–285 (2011).
-
Racine, N., Plamondon, A., Mcdonald, S., Tough, S. & Madigan, S. The consistency of maternal childhood abuse reporting in pregnancy and the postpartum period. J. Womens Health 29, 561–569 (2020).
-
Shannon, C. et al. Reliability of reports of childhood trauma in bipolar disorder: a test–retest study over 18 months. J. Trauma Dissociation 17, 511–519 (2016).
-
Simpson, S. et al. Stability of retrospective self-reports of childhood trauma in first-episode psychosis. Early Interv. Psychiatry 13, 908–913 (2019).
-
Smith, N., Lam, D., Bifulco, A. & Checkley, S. Childhood Experience of Care and Abuse Questionnaire (CECA.Q). Soc. Psychiatry Psychiatr. Epidemiol. 37, 572–579 (2002).
-
Spinhoven, P., Bamelis, L., Haringsma, R., Molendijk, M. & Arntz, A. Consistency of reporting sexual and physical abuse during psychological treatment of personality disorder: an explorative study. J. Behav. Ther. Exp. Psychiatry 43, S43–S50 (2012).
-
Teicher, M. H. & Parigger, A. The ‘Maltreatment and Abuse Chronology of Exposure’ (MACE) scale for the retrospective assessment of abuse and neglect during development. PLoS ONE 10, e0117423 (2015).
-
Wielaard, I., Stek, M. L., Comijs, H. C. & Rhebergen, D. Reliability of retrospective reports on childhood abuse and its determinants in older adults during a 6-year follow-up. J. Psychiatr. Res. 105, 9–16 (2018).
-
Xiang, Z., Liu, Z., Cao, H., Wu, Z. & Long, Y. Evaluation on long-term test–retest reliability of the Short-Form Childhood Trauma Questionnaire in patients with schizophrenia. Psychol. Res. Behav. Manag. 14, 1033–1040 (2021).
-
Zanotti, D. C. et al. An examination of the test–retest reliability of the ACE-SQ in a sample of college athletes. Psychol. Trauma Theory Res. Pract. Policy 10, 559–562 (2018).
-
Zhang, J. et al. Factor analysis and evaluation of one-year test-retest reliability of the 33-item Childhood Trauma Questionnaire in Chinese adolescents. Front. Psychol. 15, Article 1384807 (2024).
-
Murphy, E., Wickramaratne, P. & Weissman, M. The stability of parental bonding reports: a 20-year follow-up. J. Affect. Disord. 125, 307–315 (2010).
-
Breit, M., Scherrer, V., Tucker-Drob, E. M. & Preckel, F. The stability of cognitive abilities: a meta-analytic review of longitudinal studies. Psychol. Bull. 150, 399–439 (2024).
-
Matt, G. E., Vázquez, C. & Campbell, W. K. Mood-congruent recall of affectively toned stimuli: a meta-analytic review. Clin. Psychol. Rev. 12, 227–255 (1992).
-
Roozendaal, B., McEwen, B. S. & Chattarji, S. Stress, memory and the amygdala. Nat. Rev. Neurosci. 10, 423–433 (2009).
-
Proctor, L. J. & Dubowitz, H. in Handbook of Child Maltreatment Vol. 2 (eds Korbin, J. E. & Krugman, R. D.) 27–61 (Springer, 2014).
-
Stowman, S. A. & Donohue, B. Assessing child neglect: a review of standardized measures. Aggress. Violent Behav. 10, 491–512 (2005).
-
Larkina, M., Merrill, N. A. & Bauer, P. J. Developmental changes in consistency of autobiographical memories: adolescents’ and young adults’ repeated recall of recent and distance events. Memory 25, 1036–1051 (2017).
-
Wardell, V. & Palombo, D. J. Stability and malleability of emotional autobiographical memories. Nat. Rev. Psychol. 3, 393–406 (2024).
-
Roberts, B. W. & DelVecchio, W. F. The rank-order consistency of personality traits from childhood to old age: a quantitative review of longitudinal studies. Psychol. Bull. 126, 3–25 (2000).
-
Danese, A. & Widom, C. S. Associations between objective and subjective experiences of childhood maltreatment and the course of emotional disorders in adulthood. JAMA Psychiatry 80, 1009–1016 (2023).
-
Agnew-Blais, J. & Danese, A. Childhood maltreatment and unfavourable clinical outcomes in bipolar disorder: a systematic review and meta-analysis. Lancet Psychiatry 3, 342–349 (2016).
-
Nanni, V., Uher, R. & Danese, A. Childhood maltreatment predicts unfavorable course of illness and treatment outcome in depression: a meta-analysis. Am. J. Psychiatry 169, 141–151 (2012).
-
Cohen, J. A. & Mannarino, A. P. Trauma-focused cognitive behavioural therapy for children and parents. Child Adolesc. Ment. Health 13, 158–162 (2008).
-
Dalgleish, T. & Hitchcock, C. Transdiagnostic distortions in autobiographical memory recollection. Nat. Rev. Psychol. 2, 166–182 (2023).
-
Lewis, S. J. et al. The epidemiology of trauma and post-traumatic stress disorder in a representative cohort of young people in England and Wales. Lancet Psychiatry 6, 247–256 (2019).
-
Sawyer, S. M., Azzopardi, P. S., Wickremarathne, D. & Patton, G. C. The age of adolescence. Lancet Child Adolesc. Health 2, 223–228 (2018).
Funding
O.C. is funded by Mental Health Research UK. D.S. received support from the NIHR Biomedical Research Centre at South London and Maudsley National Health Service (NHS) Foundation Trust and King’s College London. A.D. received funding from the National Institute for Health Research Biomedical Research Centre at South London, Maudsley NHS Foundation Trust (NIHR203318) and King’s College London, and was supported by the Medical Research Council (P005918). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders or institutions. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the paper.
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Mental Health thanks Elsa Gewehr, Tirill F. Hjuler, Alex Lau-Zhu and Jianjian Qin for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Coleman, O., Al-Jaber, M., Aponsu, G. et al. Stability of childhood maltreatment self-reports: a systematic review and meta-analysis. Nat. Mental Health (2026). https://doi.org/10.1038/s44220-026-00677-7
-
Received:
-
Accepted:
-
Published:
-
Version of record:
-
DOI: https://doi.org/10.1038/s44220-026-00677-7
Leave a Reply