Abstract
Long COVID has been an important health concern in children and adolescents, yet factors associated with its development remain incompletely understood. Selective serotonin reuptake inhibitors (SSRIs) and serotonin–norepinephrine reuptake inhibitors (SNRIs) are widely prescribed for pediatric neuropsychiatric conditions and may influence immune and autonomic pathways involved in postinfectious symptoms. Here we show associations between SSRI/SNRI use and long coronavirus disease (COVID)-related outcomes in a retrospective cohort of 110,955 children and adolescents with pre-existing neuropsychiatric conditions across 37 US health systems participating in the National Institutes of Health Researching COVID to Enhance Recovery consortium. SSRI/SNRI use was not associated with clinician-recorded long COVID diagnosis but showed heterogeneous associations with individual symptoms. Lower risks were observed for some symptoms, including fever, chills and hair loss, whereas higher risks were observed for neurological and systemic outcomes, including postural orthostatic tachycardia syndrome, cognitive dysfunction and fatigue. These findings suggest that antidepressant exposure may be associated with differing post-COVID symptom patterns in youth and warrant further investigation.
Similar content being viewed by others
Main
Long coronavirus disease (COVID), or postacute sequelae of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection (PASC), is increasingly recognized as a substantial public health concern, including among pediatric populations. It is provisionally defined as a condition characterized by symptoms that persist for at least 3 months after acute SARS-CoV-2 infection and are not explained by alternative diagnoses1. Symptoms vary widely and may include fatigue, brain fog, dyspnea, autonomic dysfunction and neuropsychiatric complaints such as depression and anxiety1,2,3. Although most research has focused on adult populations, emerging evidence suggests that children and adolescents can also develop long COVID, albeit with potentially distinct symptom patterns4,5,6,7,8,9,10,11,12,13,14,15.
According to data from the National Center for Health Statistics in 2022, 1.3% of US children were reported to have experienced long COVID, and 0.5% had symptoms at the time of the survey16. Adolescents aged 12–17 years were more likely than younger children to report long COVID and prevalence varied by sex and race/ethnicity16. Given the developmental implications of persistent symptoms during childhood and adolescence, a better understanding of risk factors and potential modifiers of long COVID in this population, including neuropsychiatric conditions and their treatment with medications, is urgently needed.
Selective serotonin reuptake inhibitors (SSRIs) and serotonin–norepinephrine reuptake inhibitors (SNRIs) are widely used in pediatric populations to manage mood, anxiety and other neuropsychiatric disorders17. SSRIs/SNRIs have been hypothesized to mitigate the risk of long COVID through several potential mechanisms. These include anti-inflammatory and immunomodulatory properties, antiplatelet activity that may reduce COVID 2019 (COVID-19)-related microthrombosis and serotonergic modulation that may address postviral fatigue and cognitive symptoms associated with a hyposerotonergic state18,19,20. In adult populations, several observational studies and clinical trials (for example, the TOGETHER trial and STOP COVID) have suggested that fluvoxamine and other SSRIs may reduce COVID-19 (refs. 21,22,23,24,25). However, data on the effects of these agents in pediatric patients, particularly those taking SSRIs/SNRIs before infection, remain limited.
This knowledge gap is particularly relevant for children and adolescents with neuropsychiatric conditions, who may be more vulnerable to both SARS-CoV-2 infection and its postacute sequelae owing to biological susceptibility and healthcare disparities26,27. Furthermore, millions of youth are prescribed SSRIs or SNRIs chronically28, raising critical questions about whether these medications may alter the risk of developing long COVID after infection.
While biologically plausible mechanisms support a potential protective role for SSRIs/SNRIs, prior epidemiologic studies in pediatric populations have not adequately addressed this question. To address this gap, we conducted a large-scale retrospective cohort study using electronic health record (EHR) data from the Researching COVID to Enhance Recovery (RECOVER) consortium to evaluate the association between SSRI/SNRI use and new-onset long COVID manifestations in children and adolescents with documented neuropsychiatric conditions.
Results
Cohort identification and baseline characteristics
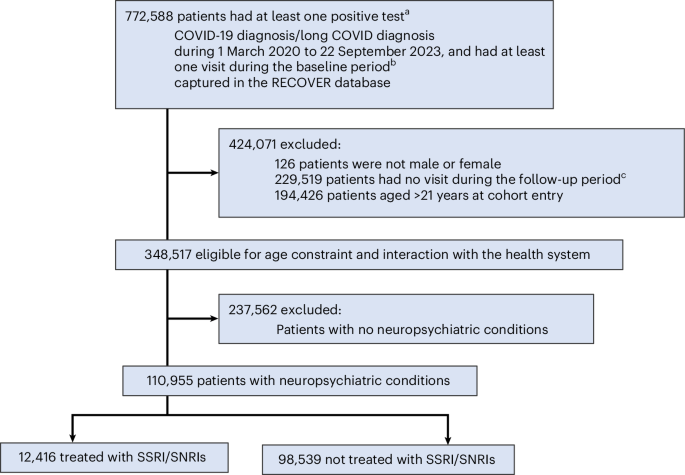
Among 110,955 pediatric patients aged 5–20 years with a documented SARS-CoV-2 infection and pre-existing neuropsychiatric conditions met the inclusion criteria (Fig. 1). Of these, 12,416 (11.2%) were prescribed an SSRI/SNRI before infection and 98,539 (88.8%) were not. Long COVID outcomes were evaluated during a standardized 28–179-day period after infection to ensure equal observational time across participants.
Baseline characteristics are summarized in Table 1. The SSRI/SNRI group had a higher proportion of female patients (68.7% versus 50.6%) and older adolescents aged 16–20 years (55.9% versus 34.0%) compared with the non-SSRI/SNRI group. Racial and ethnic distribution also differed: non-Hispanic white patients comprised a greater share of the SSRI/SNRI group (68.4% versus 47.3%), while non-Hispanic Black patients (8.6% versus 18.1%) and Hispanic patients (13.2% versus 22.8%) were under-represented.
Acute COVID-19 severity was comparable across groups: 55.4% and 55.9% of participants in the SSRI/SNRI and non-SSRI/SNRI groups, respectively, were asymptomatic, and 34.2% and 35.6% had mild disease in the SSRI/SNRI and non-SSRI/SNRI groups, respectively. Chronic disease burden was slightly higher among the SSRI/SNRI users (noncomplex, 36.2%; complex, 34.6%) relative to the non-SSRI/SNRI users (29.4% and 30.3%, respectively). A larger proportion of the SSRI/SNRI group had received ≥2 COVID-19 vaccine doses before infection (46.6% versus 37.3%).
Table 2 presents the distribution of neuropsychiatric conditions. Anxiety disorder (73.0% versus 32.6%) and major depression (47.3% versus 14.5%) were higher in the SSRI/SNRI group. Communication/motor disorder (14.3% versus 4.8%) and autism spectrum disorder (10.4% versus 9.5%) were more prevalent among nonusers. Within the SSRI/SNRI cohort, 90.7% received SSRIs and 9.3% received SNRIs. SNRI use was more common among patients with specific diagnoses, including hypersomnia (25.2%), opioid-related substance use disorder (23.4%) and personality disorders (23.2%). By contrast, SNRI use was less frequent among patients with intellectual disability (3.9%) and communication/motor disorder (4.2%), suggesting diagnosis-specific variability in pharmacologic selection.
Incidence of long COVID outcomes
The incidence of long COVID was expressed as the proportion of at-risk individuals who developed each outcome within the fixed follow-up window. The diagnosis code U09.9, indicative of long COVID, was recorded in 1.13% of the SSRI/SNRI group and 0.79% of the non-SSRI/SNRI group (Table 3). However, when examining a broader composite of 23 predefined long COVID symptoms/conditions, the SSRI/SNRI group had a lower incidence (10.13%) compared with the non-SSRI/SNRI group (18.14%). This unexpected inverse association suggests potentially complex interactions between pre-infection SSRI/SNRI use and symptom manifestation.
Symptom/condition-specific analyses revealed important differences. Fatigue and malaise occurred more frequently in the SSRI/SNRI group (4.24%) than in the non-SSRI/SNRI group (2.59%). Similarly, postural orthostatic tachycardia syndrome (POTS) was more common in the SSRI/SNRI group (3.51% versus 1.82%). Other symptoms/conditions with a higher incidence in the SSRI/SNRI group included headache (4.63% versus 3.74%), generalized pain (2.94% versus 1.93%) and arrhythmia (3.05% versus 2.22%). Respiratory symptoms, however, were slightly lower in the SSRI/SNRI group (7.25% versus 8.18%). Additional symptom incidence and drug-specific breakdowns are provided in Table 3 and Supplementary Tables 3 and 4.
Adjusted risk estimates for long COVID events
Figure 2 shows the results from the propensity score-adjusted analyses. SSRI/SNRI use was not significantly associated with long COVID diagnosis as defined by the U09.9 code (relative risk (RR) 1.12; 95% confidence interval (CI) 0.92–1.36). However, SSRI/SNRI use was associated with a significantly higher RR of experiencing any of the 23 long COVID symptoms/conditions collectively (RR 1.56, 95% CI 1.23–1.99). Specifically, reduced risks were observed for fever and chills (RR 0.86, 95% CI 0.75–0.99) and hair loss (RR 0.69, 95% CI 0.49–0.96) among SSRI/SNRI users. Conversely, increased risks were observed for thromboembolic events (RR 1.93, 95% CI 1.35–2.77), cognitive dysfunction (RR 1.84, 95% CI 1.39–2.43), POTS (RR 1.33, 95% CI 1.18–1.51), abnormal liver enzymes (RR 1.33, 95% CI 1.02–1.73), fatigue and malaise (RR 1.20, 95% CI 1.07–1.34), generalized pain (RR 1.19, 95% CI 1.05–1.35) and abdominal pain (RR 1.13, 95% CI 1.03–1.25).
Subgroup and sensitivity analyses
Findings were consistent across subgroup and sensitivity analyses (Supplementary Tables 5–18). Negative control outcome analysis for 26 negative control outcomes yielded no significant associations, supporting the robustness of the results and suggesting minimal unmeasured confounding (Supplementary Table 19).
Discussion
This large retrospective study identified complex and symptom/condition-specific associations between pre-infection SSRI/SNRI use and long COVID manifestations in pediatric patients with neuropsychiatric conditions. Although the SSRI/SNRI group demonstrated a lower overall incidence of any of the 23 long COVID symptoms/conditions (10.13% versus 18.14%), symptom/condition-specific analyses revealed higher risks for certain neurological and autonomic symptoms/conditions, such as POTS and cognitive dysfunction, and lower risks for fever, chills and hair loss.
Although both groups had overlapping neuropsychiatric diagnoses, the likelihood of receiving SSRIs/SNRIs appeared to depend on multiple factors, including symptom severity, functional impairment, clinician practice patterns and parental preferences. SSRIs/SNRIs are often initiated in cases of moderate-to-severe depression and anxiety, while conditions such as autism spectrum disorders, which are more prevalent in the non-SSRI/SNRI group, are typically managed with alternative interventions such as stimulants or behavioral therapies29,30. These treatment selection patterns underscore the importance of accounting for confounding by indication in analyses involving psychotropic medications31.
The temporal sequencing in this study, where exposure to SSRIs/SNRIs precedes SARS-CoV-2 infection, mitigates reverse causation and ensures that medication effects were present during the acute and early postacute phases when long-COVID-related biological processes emerge. This timing strengthens the plausibility that SSRIs/SNRIs could influence downstream symptom development through their known immunomodulatory and autonomic effect. Duloxetine, for example, is approved for pediatric generalized anxiety disorder and is also used off label for chronic pain, making its post-COVID associations particularly relevant32,33. Given the known immunomodulatory properties of SSRIs, including reduced production of pro-inflammatory cytokines and alterations in platelet activity and autonomic tone, their use during viral illness may influence symptom trajectories differently depending on the postinfectious phenotype.
Although this study focuses on a pediatric cohort, findings from adult studies provide relevant context. PASC, including POTS and myalgic encephalomyelitis/chronic fatigue syndrome, have been increasingly reported in adults, particularly women34,35. While pediatric and adult cases differ in prevalence and pathophysiologic features, our observed associations between SSRI/SNRI exposure and increased POTS and fatigue in youth may reflect neuroimmune or autonomic mechanisms35,36,37. The increased POTS risk probably reflects underlying dysautonomia, especially in adolescent females, and may be exacerbated postinfection35,38,39,40. Catatonia, which also involves autonomic instability, may contribute to this symptom profile. Although SSRIs and SNRIs have been associated with dysautonomic effects in rare cases, catatonia is more often associated with underlying neuropsychiatric, autoimmune or infectious etiologies41,42. It remains underdiagnosed in pediatric populations and may be variably coded in clinical records41,43.
These findings should be interpreted with caution. SSRIs and SNRIs are established treatments for pediatric neuropsychiatric conditions, which are pre-existing conditions by virtue of our study design, and are generally safe and effective when prescribed appropriately44. Untreated psychiatric disorders carry substantial risks, including suicidal ideation and behavior, functional impairment and increased mortality. Causal inferences should not be made without considering the underlying condition, which may itself predispose patients to adverse postinfectious outcomes. The SSRI/SNRI-exposed group demonstrated slightly higher rates of COVID-19 vaccination. This difference should not be interpreted as vaccine-related harm, particularly given the robust evidence that vaccination reduces the risk of long COVID6. Misinterpretation may contribute to vaccine hesitancy and public health risk.
These findings both align with and differ from previous research on SSRI/SNRI use in COVID-19. Adult studies, including the TOGETHER24 and STOP-COVID25 trials, have shown that SSRIs, particularly fluvoxamine, may reduce hospitalization and inflammatory markers. However, our pediatric results show a more nuanced pattern: while SSRI/SNRI users had lower overall long COVID symptom incidence, they exhibited elevated risks for specific neurological outcomes. These differences may reflect age-related neuroimmune responses, altered blood–brain barrier (BBB) integrity or distinct pharmacologic effects in developing brains. Unlike adults, pediatric findings suggest symptom-specific variations that warrant further study.
Previous pediatric studies have primarily addressed the psychological impact of the pandemic rather than medication-specific associations with long COVID27,45. These findings bridge this gap and underscore important demographic considerations. The over-representation of female and white participants in the SSRI/SNRI group reflects known disparities in pediatric mental healthcare access and utilization and may limit the generalizability of findings to under-represented populations.
SARS-CoV-2 infection may compromise BBB integrity, increasing permeability and allowing greater central nervous system penetration of substances46,47. This disruption may lead to higher concentrations of SSRIs and SNRIs at the presynaptic axonal terminals of neurons, potentially exacerbating neurological symptoms associated with long COVID48,49. Infection-induced oxidative stress and basement membrane damage may impair BBB function even without disrupting tight junctions50,51. In addition, altered activity of transporters such as P-glycoprotein may affect antidepressant distribution and clearance18. These mechanisms may partly explain the elevated neurologic symptom risk observed in treated patients. Further studies are needed to clarify the impact of BBB dysfunction on SSRI/SNRI effects during post-COVID recovery.
This study has several methodological strengths that support the validity and generalizability of the findings. The RECOVER consortium’s multicenter EHR database enabled analysis of a large, diverse pediatric population and enabled robust subgroup evaluations. The use of propensity score stratification and extensive covariate adjustment helped reduce confounding31, and the inclusion of negative control outcomes improved bias calibration52,53. In addition, detailed symptom/condition-specific analysis offered clinically relevant granularity.
However, several limitations must be considered. The retrospective design and reliance on EHR data may lead to misclassification of infection status or outcomes. Residual confounding is possible despite statistical adjustment, particularly from unmeasured factors such as socioeconomic status or family psychiatric history. Differences in healthcare utilization between groups may influence the documentation of symptoms and diagnoses. In addition, the absence of chart validation and the evolving definitions of long COVID may impact interpretability. Importantly, the observed SSRI/SNRI use rate (11.2%) exceeded national estimates of pediatric antidepressant use (~4.8%)54, though antidepressant dispensing to youth rose 63.5% after the COVID-19 outbreak28. This difference may limit generalizability, but it reflects the study’s intended target population. Although our design excluded patients with documented baseline symptoms from outcome-specific analyses and adjusted for all pre-existing neuropsychiatric diagnoses, we acknowledge that some conditions, such as encephalopathy, exhibit fluctuating courses that may not be fully captured in EHR data. As such, symptom recurrence after infection may be difficult to distinguish from true incident post-COVID manifestations, and this limitation may partially contribute to the differential risks observed for neurologic and autonomic outcomes.
This large-scale retrospective analysis reveals complex associations between SSRI/SNRI use and long COVID manifestations in pediatric patients with neuropsychiatric conditions. While suggesting overall lower long COVID symptom occurrence in SSRI/SNRI users, this study identifies important symptom/condition-specific risks that warrant careful consideration in clinical practice. These findings underscore the need for personalized risk assessment and monitoring in pediatric patients with neuropsychiatric conditions who used SSRIs/SNRIs during the COVID-19 pandemic.
Methods
Data sources and cohort construction
This retrospective cohort study was approved by the Biomedical Research Alliance of New York Institutional Review Board (protocol no. 21-08-508) with a waiver of informed consent and Health Insurance Portability and Accountability Act authorization. The Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines were followed. This analysis was conducted as part of the National Institutes of Health (NIH) RECOVER Initiative, which seeks to understand, treat and prevent PASC (https://recovercovid.org/). Overall, 37 US children’s hospitals and healthcare systems contributed EHR data (Supplementary Note 1).
This study spanned from 1 March 2020 to 19 March 2024. Cohort entry occurred between 1 March 2020 and 22 September 2023, allowing a minimum of 179 days of follow-up for long COVID assessment. Patients were eligible if they were older than 5 years and younger than 21 years, had a documented SARS-CoV-2 infection during the cohort entry period and had a pre-existing neuropsychiatric condition7. Individuals were required to have at least one healthcare encounter during a baseline period (24 months to 7 days before SARS-CoV-2 infection) and at least one encounter during the standard follow-up period (28–179 days after SARS-CoV-2 infection). SARS-CoV-2 infection was defined by a positive PCR, serologic or antigen test, or by a clinician-documented COVID-19 diagnosis. The index date was defined as the date of the first recorded SARS-CoV-2 infection during the study period. Detailed information on data processing, cohort construction and the definition of neuropsychiatric conditions is available in Supplementary Notes 2–4. Figure 1 shows the selection of participants for the SSRI/SNRI and non-SSRI/SNRI groups.
Participant selection from the NIH RECOVER pediatric cohort. Children and adolescents aged 5–20 years with documented SARS-CoV-2 infection between 1 March 2020 and 22 September 2023 and with pre-existing neuropsychiatric conditions were identified. Individuals were required to have at least one healthcare encounter during the baseline period (24 months to 7 days before infection) and at least one encounter during the follow-up period (28–179 days after the index date). The index date was defined as the first recorded SARS-CoV-2 infection during the study period. Participants were classified according to exposure to SSRIs or SNRIs during the exposure window spanning 28 days before to 28 days after infection. The final analytic cohort included 110,955 participants, comprising 12,416 SSRI/SNRI users and 98,539 nonusers. aIncluding PCR, antigen, serology tests; b7–18 months before the index date; c28–179 days after the index date.
RRs and 95% CIs for long COVID-related outcomes comparing patients receiving SSRI/SNRI treatment with those not receiving SSRI/SNRI treatment. RRs were estimated using modified Poisson regression models following propensity score stratification based on baseline covariates. The squares represent point estimates, and the horizontal lines indicate 95% CIs. CIs extending beyond the plotting range are truncated at an RR of 3. The vertical dotted line indicates no association (RR of 1). The horizontal dashed line separates outcome groups. The unit of analysis was the individual participant. The analytic cohort included 110,955 patients (12,416 SSRI/SNRI users and 98,539 nonusers). Each outcome was evaluated among participants without prior documentation of the corresponding condition during the baseline period. sx, symptoms.
Exposure definition
SSRIs included citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine and sertraline. SNRIs included desvenlafaxine, duloxetine and venlafaxine. Patients were classified as SSRI/SNRI users if they received treatment during the period spanning 28 days before to 28 days after the index date, based on established pediatric prescribing practices and published research55. All others were classified as non-SSRI/SNRI.
Long COVID outcome definitions
To identify long COVID outcomes, the study used two complementary definitions grounded in clinical practice and established pediatric research. The primary definition relied on the presence of a clinician-recorded diagnosis using the International Classification of Diseases, Tenth Revision, Clinical Modification code U09.9, a coding designation that has gained widespread adoption for identifying post-COVID conditions. The second definition included a list of symptoms and clinical conditions potentially linked to pediatric long COVID, as determined by expert pediatric consensus and prior studies13,56, including abdominal pain, abnormal liver enzymes, acute kidney injury, acute respiratory distress syndrome, arrhythmias, cardiovascular signs and symptoms, changes in taste and smell, chest pain, cognitive dysfunction, fatigue and malaise, fever and chills, fluid and electrolyte imbalances, generalized pain, hair loss, headache, heart disease, musculoskeletal pain, myocarditis, myositis, POTS or dysautonomia, respiratory signs and symptoms, skin symptoms, thrombophlebitis and thromboembolism (Supplementary Table 1). These outcomes were assessed during the harmonized follow-up period of 28–179 days after the index date and only among patients without prior documentation of the same conditions during the baseline period.
Patient-specific covariates
Baseline characteristics were collected before or at the time of SARS-CoV-2 infection. These included demographic variables, including age at index date, sex (female or male) and race/ethnicity (Asian American/Pacific Islander, Hispanic, non-Hispanic Black, non-Hispanic white, multiple or other/unknown); clinical variables, including obesity status, a chronic condition indicator defined by the Pediatric Medical Complexity Algorithm (no chronic condition, noncomplex chronic condition or complex chronic condition)57, and a list of pre-existing chronic conditions; healthcare utilization in the baseline period, including the number of inpatient, outpatient, emergency department visits, the number of unique medications, and the number of negative SARS-CoV-2 tests (0, 1, 2 or ≥3); vaccine status, including dosage of COVID-19 vaccine received before infection (0, 1 or ≥2) and the time since most recent vaccination (no vaccine, <4 months or ≥4 months); calendar year-month of index infection; severity of acute COVID-19 (categorized as asymptomatic, mild, moderate, or severe) based on COVID-19-related hospitalization, intensive care unit admission, respiratory support procedures and diagnosis codes indicating respiratory acute COVID-19 complications within 14 days of the index date58; and indicators for the 37 data-contributing sites.
Statistical analysis
The incidence of long COVID outcomes was calculated for the SSRI/SNRI and control groups as the proportion of at-risk patients (excluding those with the condition at baseline) who develop the outcome during follow-up. Because all participants contributed data over a fixed observation window and outcomes were based on clinician-documented events, this approach would not alter the interpretation of incidence.
To address confounding, we applied propensity score stratification based on covariates measured before the index date. Covariate balance after stratification was evaluated using standardized mean differences, with a standardized mean difference of ≤0.1 considered acceptable59. Adjusted RRs and 95% CIs for each outcome were estimated using modified Poisson regression models60. Statistical methods are described in Supplementary Note 5.
Secondary analysis
Prespecified subgroup analyses were conducted by age group (5–11, 12–15 and 16–20 years), sex (female or male), race and ethnicity (non-Hispanic Black, non-Hispanic white, and Hispanic)5, obesity status (obese versus non-obese)4,15 and severity of acute COVID-19 (nonsevere (asymptomatic or mild) versus severe (moderate or severe)).
Sensitivity analyses were conducted to assess the robustness of findings. These included the exclusion of participants with neuropsychiatric diagnoses that are infrequently treated with SSRIs/SNRIs in children and adolescents, as well as the exclusion of individuals with COVID-19 index dates before the implementation of the International Classification of Diseases, Tenth Revision, Clinical Modification U09.9 code on 1 October 2021. In addition, negative control outcome analyses were performed to calibrate residual bias arising from unmeasured confounding and systematic error52,53. A set of 26 negative control outcomes, selected by board-certified pediatricians (Supplementary Table 2), was used under the assumption of no association with SSRI/SNRI exposure.
All analyses were performed using R version 4.4.0 (R Project for Statistical Computing). A two-sided P value <0.05 was considered statistically significant. Analyses were conducted from December 2024 to March 2025.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The results reported in this study are based on detailed individual-level patient data compiled as part of the RECOVER program. Owing to the high risk of re-identification based on the number of unique patterns in the data, patient privacy regulations prohibit us from releasing the data publicly. The data are maintained in a secure enclave, with access managed by the program coordinating center, to remain compliant with regulatory and program requirements. Please direct requests to access the data, either for reproduction of the work reported here or for other purposes, to the RECOVER EHR Pediatric Coordinating Center (email: recover@chop.edu). Source data are provided with this paper.
Code availability
The code used for the analysis in this study is available via Code Ocean at https://doi.org/10.24433/CO.4519602.v1.
References
-
Soriano, J. B., Murthy, S., Marshall, J. C., Relan, P. & Diaz, J. V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 22, e102–e107 (2022).
-
Buonsenso, D. et al. Preliminary evidence on long COVID in children. Acta Paediatr. 110, 2208–2211 (2021).
-
Stephenson, T. et al. Long COVID and the mental and physical health of children and young people: national matched cohort study protocol (the CLoCk study). BMJ Open 11, e052838 (2021).
-
Zhou, T. et al. Body mass index and postacute sequelae of SARS-CoV-2 infection in children and young adults. JAMA Netw. Open 7, e2441970 (2024).
-
Zhang, D. et al. Racial/ethnic differences in post-acute sequelae of SARS-CoV-2 in children and adolescents in the United States. Nat. Commun. 16, 878 (2025).
-
Wu, Q. et al. Real-world effectiveness and causal mediation study of BNT162b2 on long COVID risks in children and adolescents. EClinicalMedicine 79, 102962 (2025).
-
Lu, Y. et al. Risk of neuropsychiatric and related conditions associated with SARS-CoV-2 infection: a difference-in-differences analysis. Nat. Commun. 16, 6829 (2025).
-
Zhang, D. et al. Pediatric gastrointestinal tract outcomes during the postacute phase of COVID-19. JAMA Netw. Open 8, e2458366 (2025).
-
Li, L. et al. Kidney function following COVID-19 in children and adolescents. JAMA Netw. Open 8, e254129 (2025).
-
Wu, Q. et al. Real-world effectiveness of BNT162b2 against infection and severe diseases in children and adolescents. Ann. Intern. Med. 177, 165–176 (2024).
-
Zhang, B. et al. Long COVID associated with SARS-CoV-2 reinfection among children and adolescents in the omicron era (RECOVER-EHR): a retrospective cohort study. Lancet Infect. Dis. https://doi.org/10.1016/S1473-3099(25)00476-1 (2025).
-
Gross, R. S. et al. Characterizing long COVID in children and adolescents. JAMA 332, 1174–1188 (2024).
-
Rao, S. et al. Clinical features and burden of postacute sequelae of SARS-CoV-2 infection in children and adolescents. JAMA Pediatr. 176, 1000–1009 (2022).
-
Lei, Y. et al. Post-acute dyslipidemia and abnormal Body Mass Index in children and adolescents with COVID-19: a cohort study from the RECOVER Initiative. J. Pediatr. https://doi.org/10.1016/j.jpeds.2026.114996 (2026)
-
Zhou, T. et al. Pre-COVID-19 body mass index and post-acute cardiovascular, gastrointestinal, and neuropsychiatric outcomes among children and young adults with SARS-CoV-2 infection: an EHR-based cohort study from the RECOVER Initiative. J. Infect. 92, 106702 (2026).
-
Vahratian, A., Adjaye-Gbewonyo, D., Lin, J.-M. S. & Saydah, S. Long COVID in children: United States, 2022. NCHS https://www.cdc.gov/nchs/products/databriefs/db479.htm (2023).
-
Walkup, J. T. Antidepressant efficacy for depression in children and adolescents: industry- and NIMH-funded studies. Am. J. Psychiatry 174, 430–437 (2017).
-
Kealy, J., Greene, C. & Campbell, M. Blood–brain barrier regulation in psychiatric disorders. Neurosci. Lett. 726, 133664 (2020).
-
Bonnet, U., Juckel, G. & Kuhn, J. Antidepressants for prevention of severe COVID-19, long COVID and outlook for other viral diseases. Front. Med. 11, 1305184 (2024).
-
Hashimoto, Y., Suzuki, T. & Hashimoto, K. Mechanisms of action of fluvoxamine for COVID-19: a historical review. Mol. Psychiatry 27, 1898–1907 (2022).
-
Visos-Varela, I. et al. Repurposing selective serotonin reuptake inhibitors for severity of COVID-19: a population-based study. Eur. Neuropsychopharmacol. 71, 96–108 (2023).
-
Sidky, H. et al. Assessing the effect of selective serotonin reuptake inhibitors in the prevention of post-acute sequelae of COVID-19. Comput. Struct. Biotechnol. J. 24, 115–125 (2024).
-
Hoertel, N. et al. Association between antidepressant use and reduced risk of intubation or death in hospitalized patients with COVID-19: results from an observational study. Mol. Psychiatry 26, 5199–5212 (2021).
-
Reis, G. et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial. Lancet Glob. Health 10, e42–e51 (2022).
-
Lenze, E. J. et al. Fluvoxamine vs Placebo and clinical deterioration in outpatients with symptomatic COVID-19. JAMA 324, 2292–2300 (2020).
-
Peluso, M. J. et al. Markers of immune activation and inflammation in individuals with postacute sequelae of severe acute respiratory syndrome coronavirus 2 infection. J. Infect. Dis. 224, 1839–1848 (2021).
-
Racine, N. et al. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19. JAMA Pediatr. 175, 1142–1150 (2021).
-
Chua, K.-P., Volerman, A., Zhang, J., Hua, J. & Conti, R. M. Antidepressant dispensing to US adolescents and young adults: 2016–2022. Pediatrics 153, e2023064245 (2024).
-
Aman, M. G., Farmer, C. A., Hollway, J. & Arnold, L. E. Treatment of inattention, overactivity, and impulsiveness in autism spectrum disorders. Child Adolesc. Psychiatr. Clin. N. Am. 17, 713–738 (2008).
-
Ginsburg, G. S., Riddle, M. A. & Davies, M. Somatic symptoms in children and adolescents with anxiety disorders. J. Am. Acad. Child Adolesc. Psychiatry 45, 1179–1187 (2006).
-
Patrick, A. R. et al. The implications of propensity score variable selection strategies in pharmacoepidemiology: an empirical illustration. Pharmacoepidemiol. Drug Saf. 20, 551–559 (2011).
-
Tynan, R. J. et al. A comparative examination of the anti-inflammatory effects of SSRI and SNRI antidepressants on LPS stimulated microglia. Brain Behav. Immun. 26, 469–479 (2012).
-
Dowlati, Y. et al. A meta-analysis of cytokines in major depression. Biol. Psychiatry 67, 446–457 (2010).
-
Komaroff, A. L. & Lipkin, W. I. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol. Med. 27, 895–906 (2021).
-
Blitshteyn, S. & Whitelaw, S. Postural orthostatic tachycardia syndrome (POTS) and other autonomic disorders after COVID-19 infection: a case series of 20 patients. Immunol. Res. 69, 205–211 (2021).
-
Raj, S. R. et al. Long-COVID postural tachycardia syndrome: an American Autonomic Society statement. Clin. Autonomic Res. 31, 365–368 (2021).
-
Dani, M. et al. Autonomic dysfunction in ‘long COVID’: rationale, physiology and management strategies. Clin. Med. 21, e63–e67 (2021).
-
Garland, E. M., Raj, S. R., Black, B. K., Harris, P. A. & Robertson, D. The hemodynamic and neurohumoral phenotype of postural tachycardia syndrome. Neurology 69, 790–798 (2007).
-
Shaw, B. H. et al. The face of postural tachycardia syndrome – insights from a large cross-sectional online community-based survey. J. Intern. Med. 286, 438–448 (2019).
-
Cantrell, C. et al. Post-COVID postural orthostatic tachycardia syndrome (POTS): a new phenomenon. Front. Neurol. 15, 1297964 (2024).
-
Benarous, X., Raffin, M., Ferrafiat, V., Consoli, A. & Cohen, D. Catatonia in children and adolescents: new perspectives. Schizophr. Res. 200, 56–67 (2018).
-
Smith, J. R. et al. Diagnostic features of paediatric catatonia: multisite retrospective cohort study. BJPsych Open 10, e96 (2024).
-
Dhossche, D. M., Wilson, C. & Wachtel, L. E. Catatonia in childhood and adolescence: Implications for the DSM-5. Prim. Psychiatry 17, 35–39 (2010).
-
Cipriani, A. et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: a network meta-analysis. Lancet 388, 881–890 (2016).
-
Ravens-Sieberer, U. et al. Quality of life and mental health in children and adolescents during the first year of the COVID-19 pandemic: results of a two-wave nationwide population-based study. Eur. Child Adolesc. Psychiatry 32, 575–588 (2023).
-
Krasemann, S. et al. The blood-brain barrier is dysregulated in COVID-19 and serves as a CNS entry route for SARS-CoV-2. Stem Cell Rep. 17, 307–320 (2022).
-
Greene, C. et al. Blood–brain barrier disruption and sustained systemic inflammation in individuals with long COVID-associated cognitive impairment. Nat. Neurosci. 27, 421–432 (2024).
-
Shinohara, R., Aghajanian, G. K. & Abdallah, C. G. Neurobiology of the rapid-acting antidepressant effects of ketamine: impact and opportunities. Biol. Psychiatry 90, 85–95 (2021).
-
Hiemke, C. et al. Consensus guidelines for therapeutic drug monitoring in neuropsychopharmacology: update 2017. Pharmacopsychiatry 51, e1 (2018).
-
Dhariwal, R., Dave, K. & Jain, M. Omics-based analysis of mitochondrial dysfunction and BBB integrity in post-COVID-19 sequelae. Sci. Rep. 14, 31016 (2024).
-
Zhang, L. et al. SARS-CoV-2 crosses the blood–brain barrier accompanied with basement membrane disruption without tight junctions alteration. Signal Transduct. Target. Ther. 6, 337 (2021).
-
Schuemie, M. J., Hripcsak, G., Ryan, P. B., Madigan, D. & Suchard, M. A. Empirical confidence interval calibration for population-level effect estimation studies in observational healthcare data. Proc. Natl Acad. Sci. USA 115, 2571–2577 (2018).
-
Schuemie, M. J., Ryan, P. B., DuMouchel, W., Suchard, M. A. & Madigan, D. Interpreting observational studies: why empirical calibration is needed to correct p-values. Stat. Med. 33, 209–218 (2014).
-
Pratt, L. A., Brody, D. J. & Gu, Q. Antidepressant use among persons aged 12 and over: United States, 2011–2014. NCHS https://www.cdc.gov/nchs/products/databriefs/db283.htm (2017).
-
Butzin-Dozier, Z. et al. SSRI use during acute COVID-19 and risk of Long COVID among patients with depression. BMC Med. 22, 445 (2024).
-
Razzaghi, H. et al. Vaccine effectiveness against long COVID in children. Pediatrics 153, e2023064446 (2024).
-
Simon, T. D. et al. Pediatric medical complexity algorithm: a new method to stratify children by medical complexity. Pediatrics 133, e1647–e1654 (2014).
-
Forrest, C. B. et al. Severity of acute COVID-19 in children <18 years old March 2020 to December 2021. Pediatrics 149, e2021055765 (2022).
-
Walker, A. et al. A tool for assessing the feasibility of comparative effectiveness research. Comp. Eff. Res. https://doi.org/10.2147/CER.S40357 (2013).
-
Zou, G. A modified Poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 159, 702–706 (2004).
Acknowledgements
This research was funded by the NIH Agreement OTA OT2HL161847-01 (to Y.C.) as part of the RECOVER research Initiative. This study is part of the NIH RECOVER Initiative, which seeks to understand, treat and prevent PASC. For more information on RECOVER, visit https://recovercovid.org/. We thank the National Community Engagement Group, all patient, caregiver and community representatives and all the participants enrolled in the RECOVER Initiative. This content is solely the responsibility of the authors and does not necessarily represent the official views of the RECOVER Initiative, the NIH or other funders. The views, statements and opinions presented in this publication are solely the responsibility of the author(s) and do not necessarily represent the views of other organizations participating in, collaborating with or funding PCORnet or of the Patient-Centered Outcomes Research Institute. Authorship has been determined according to ICMJE recommendations.
Ethics declarations
Competing interests
L.C.B. has received grants from the Patient-Centered Outcomes Research Institute. The other authors declare no competing interests.
Peer review
Peer review information
Nature Mental Health thanks Sarah L. O’Dor and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhou, T., Zhang, B., Lu, Y. et al. SSRI/SNRI and long COVID in children and adolescents with neuropsychiatric conditions: a cohort study from the RECOVER Initiative. Nat. Mental Health (2026). https://doi.org/10.1038/s44220-026-00675-9
-
Received:
-
Accepted:
-
Published:
-
Version of record:
-
DOI: https://doi.org/10.1038/s44220-026-00675-9
Leave a Reply