A 2026 Journal of Neuroinflammation review organized parasite-linked neuropsychiatric risk around 5 gut-immune-brain routes; direct CNS parasitic disease carries the clearest signal, while broader mood and cognition associations usually remain observational and confounded.[1]
Research Highlights
- 5 pathways converge on brain function: the 2026 review connected parasite exposure to peripheral cytokines, gut dysbiosis, intestinal permeability, blood-brain barrier dysfunction, and microglia/astrocyte activation.
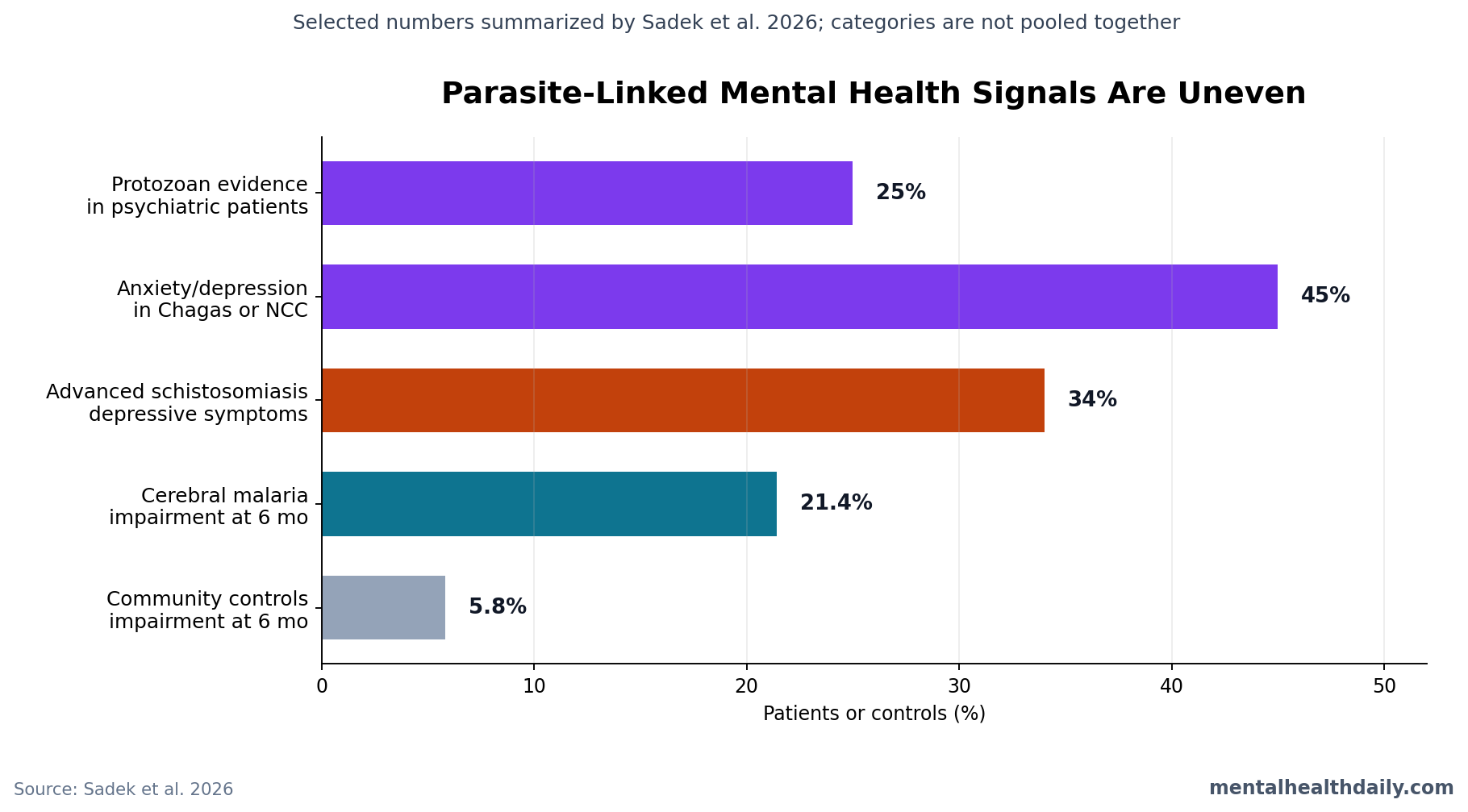
- Psychiatric-patient signal is broad: Sadek et al. cited a 2024 meta-analysis reporting protozoan-infection evidence in approximately 25% of psychiatric patients globally, with higher regional prevalence in Asia.[2]
- Neurotropic parasites show high comorbidity numbers: a developing-country meta-analysis was summarized as finding anxiety or depression in approximately 45% of patients with Chagas disease or neurocysticercosis.[3]
- Cerebral malaria has prospective follow-up evidence: 21.4% of cerebral-malaria survivors showed cognitive impairment at 6 months vs. 5.8% of community controls, and survivors were 3.7 times more likely to be impaired.[4]
- Schistosomiasis illustrates indirect risk: a 2024 China study found depressive symptoms in about 34% of advanced Schistosoma japonicum cases vs. about 22% with early-stage disease or no infection.[5]
Neuroinflammation means immune activation inside or near the nervous system, especially involving brain-resident immune cells such as microglia and support cells such as astrocytes. Parasite-linked neuroinflammation is not one mechanism. It can mean cysts in brain tissue, malaria-related injury in brain microvessels, systemic cytokines signaling into the brain, sleep disruption from infection symptoms, or gut-microbiome changes that alter immune tone.
That distinction keeps the evidence honest. A parasite can be a direct neurological disease in one context and only a weak psychiatric-risk marker in another.
Parasites Feed Into 5 Gut-Immune-Brain Routes
Sadek et al. grouped protozoa and helminths into a shared but heterogeneous framework.[1] Protozoa are single-celled parasites, including Toxoplasma gondii, Plasmodium species, and trypanosomes. Helminths are parasitic worms, including pinworms, schistosomes, Toxocara, and Taenia solium.
The review’s useful move was separating pathways rather than treating infection as a generic inflammatory blob:
- Peripheral cytokine production: cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) can drive sickness behavior, fatigue, low motivation, and sleep disruption.
- Gut dysbiosis: parasite infection can shift gut bacteria and microbial metabolites, including short-chain fatty acids (SCFAs), which help regulate intestinal barrier integrity and immune tone.
- Barrier leakage: intestinal permeability can increase immune exposure to microbial products, amplifying immune-to-brain signaling.
- Blood-brain barrier disruption: inflammatory endothelial activation can make it easier for immune signals or cells to affect brain tissue.
- Glial and neurochemical remodeling: microglia, astrocytes, dopamine, serotonin, gamma-aminobutyric acid (GABA), kynurenine metabolism, microRNAs, and epigenetic regulation can shift after infection in some models.
Evidence-strength note: the Sadek et al. paper is a narrative mechanistic review, not a new cohort, randomized trial, or meta-analysis. Its value is synthesis and mechanism-mapping. It cannot assign a population-level causal effect size for “parasites” as a single exposure.
Toxoplasma Is a Signal, Not a Standalone Psychiatric Explanation
Toxoplasma gondii is a neurotropic protozoan that can form latent tissue cysts and has long been studied in relation to schizophrenia, risk behavior, anxiety, and cognition. The 2026 review treated this literature carefully: associations exist, but they are modest, heterogeneous, and not automatically causal.[1]
One reason the topic attracts attention is biological plausibility. T. gondii can trigger gut inflammation, alter microbial composition in animal models, and engage immune pathways relevant to brain signaling. It has also been discussed as a dopamine-modulating parasite because it carries aromatic amino acid hydroxylase genes that can participate in L-DOPA biology.
Dopamine caution: the review explicitly warned against treating parasite-driven dopamine elevation as settled. Some genetic and in vivo studies do not support a simple story in which T. gondii directly raises host brain dopamine enough to explain behavior. Better wording is that dopamine-pathway interaction remains plausible and model-dependent, not proven as a universal mechanism.
Psychiatric association studies need the same restraint. The review cited Daré et al. as reporting that T. gondii or Toxocara exposure was associated with more than double the odds of schizophrenia or bipolar disorder in developing-country populations, with a pooled OR around 2.3.[3] That is a meaningful association, but seropositivity can track geography, poverty, food exposure, cat exposure, sanitation, immune status, and other risks that also shape mental-health outcomes.
Cerebral Malaria and Neurocysticercosis Are Stronger CNS Proof Points
Neurocysticercosis occurs when larval Taenia solium cysts lodge in the central nervous system after fecal-oral exposure to tapeworm eggs. Sadek et al. cited approximately 50 million infected individuals and around 50,000 deaths annually for cysticercosis burden, with the highest burden in endemic regions of Latin America, Africa, and Asia.[1]
This is not a subtle serology signal. Cysts in brain tissue can provoke local inflammation, blood-brain barrier disruption, raised intracranial pressure, seizures, headaches, cognitive deficits, confusion, depression, anxiety, hallucinations, and personality or behavioral change. Lesion number, stage, degeneration, and location matter, so psychiatric symptoms are not uniform. Still, neurocysticercosis provides direct proof that a parasite can become a neurological and neuropsychiatric disease.
Cerebral malaria is another high-confidence pathway. In severe Plasmodium falciparum malaria, infected red blood cells sequester in brain microvasculature, activating endothelium, disrupting the blood-brain barrier, driving cytokine release, and injuring neural tissue. Sadek et al. summarized evidence that 20-30% of children surviving cerebral malaria have persistent cognitive or behavioral deficits.[1]
A prospective Ugandan cohort made that concrete: 21.4% of cerebral-malaria survivors had significant cognitive impairment at 6 months compared with 5.8% of community controls, and adjusted analyses found survivors were 3.7 times more likely to show measurable impairment.[4] Follow-up studies also linked severe malaria to internalizing symptoms such as anxiety and withdrawn/depressed behavior, plus externalizing problems such as aggression and hyperactivity.
Schistosomiasis, Pinworm, and Toxocara Point to Indirect Paths
Schistosomiasis is caused by blood flukes of the genus Schistosoma. The mental-health pathway can be direct when eggs reach the spinal cord or brain, but the more common pathway is probably systemic: chronic organ disease, inflammation, anemia, poverty, functional impairment, and gut-liver-brain signaling.
In a 2024 Chinese study cited by the review, approximately 34% of patients with advanced Schistosoma japonicum infection had clinically significant depressive symptoms, compared with about 22% of people with early-stage disease or no infection.[5] Comorbid serious illness and personal economic hardship were major predictors of moderate to severe depression, which keeps the interpretation grounded: infection burden, disability, and social context travel together.
Enterobius vermicularis, or pinworm, shows a more ordinary but clinically believable pathway. Children with enterobiasis in a Taiwanese nationwide cohort had higher odds of anxiety disorders, depressive disorders, and sleep disturbances than uninfected peers.[6] Nocturnal itching can disrupt sleep, then sleep loss can feed irritability, fatigue, concentration problems, and mood symptoms. Microbiome effects may contribute, but the sleep pathway currently has the clearer clinical logic.
Toxocara infection, usually acquired from dog or cat roundworms, has been linked to selected cognitive-performance differences in cross-sectional studies and to memory impairment in animal neurotoxocariasis models. This line of evidence is biologically plausible because larvae can migrate into tissues and provoke eosinophil-rich inflammation, but human causality and effect size remain unsettled.
Parasite-Mental Health Research Has 4 Recurring Confounders
Parasite exposure is rarely randomly distributed. The review’s global-health sections are important because they prevent a purely mechanistic reading from becoming naive.
- Poverty and sanitation: exposure often tracks water quality, crowding, animal contact, sewage systems, and access to healthcare.
- Nutrition: helminths can worsen anemia, micronutrient deficiency, growth, and school performance, while undernutrition can increase infection severity.
- Polyparasitism: many endemic settings involve multiple infections at once, making single-pathogen attribution hard.
- Measurement mismatch: many studies use serology, chart diagnoses, or broad symptom scales rather than longitudinal infection timing, inflammatory biomarkers, neuroimaging, and standardized psychiatric interviews in the same people.
Interpretation: those confounders define the claim that can be made. Parasites can plausibly contribute to depression, anxiety, sleep disturbance, cognition, and psychosis-like phenotypes through infection-specific and host-response pathways.
Most evidence does not yet support routine parasite testing as a psychiatric diagnostic tool.
What Can Actually Change Clinically
The practical value is strongest where infection is clinically suspected or epidemiologically plausible. A patient with seizures, new cognitive changes, psychosis-like symptoms, severe sleep disruption, travel or migration exposure, eosinophilia, gastrointestinal symptoms, poor sanitation exposure, or residence in an endemic region may deserve infectious-disease thinking inside a neuropsychiatric workup.
Do not overgeneralize serology. A positive Toxoplasma IgG result usually indicates past exposure, not active brain disease and not a psychiatric diagnosis. The result may matter in pregnancy, immunosuppression, ocular disease, congenital infection, or selected neurological contexts, but it should not be sold as a simple explanation for common depression or anxiety.
Treat obvious infection pathways. Pinworm-related insomnia, neurocysticercosis with seizures, severe malaria recovery, schistosomiasis with functional impairment, or suspected toxocariasis requires diagnosis and treatment on infectious-disease grounds. Mental-health improvement may follow when sleep, inflammation, seizure burden, pain, anemia, or disability improves, but that is different from claiming an antiparasitic is an antidepressant.
Research needs better pairing. The next generation of studies should measure parasite exposure, infection stage, microbiome composition, cytokines, blood-brain barrier markers, neurocognitive testing, and psychiatric symptoms longitudinally. Without that pairing, the field will keep oscillating between overclaiming causality and ignoring a plausible infectious contributor.
Questions About Parasites, Neuroinflammation, and Mental Health
Can parasites cause depression or anxiety?
Some parasite infections can plausibly contribute to mood and anxiety symptoms through inflammation, sleep disruption, organ disease, pain, anemia, nutritional deficiency, or direct CNS involvement. The evidence is strongest for specific infections and contexts, not for a general claim that parasites commonly cause ordinary depression or anxiety.
Does Toxoplasma gondii cause schizophrenia?
No single-cause claim is supported. T. gondii exposure has been associated with schizophrenia and bipolar disorder in several studies and meta-analyses, including the OR around 2.3 association summarized by Sadek et al., but causality, timing, confounding, and mechanism remain unresolved.
Which parasite evidence is most clinically convincing?
Direct CNS or severe neuroinfectious syndromes are more convincing than broad serology associations. Neurocysticercosis, cerebral malaria, and late-stage African trypanosomiasis have clearer neurological pathways than latent-exposure studies of common psychiatric outcomes.
Should people with mental-health symptoms get parasite testing?
Testing should follow exposure history, symptoms, geography, immune status, eosinophilia, neurological signs, gastrointestinal findings, pregnancy status, or infectious-disease risk. Routine parasite screening for nonspecific mood symptoms would overread the current evidence.
References
- Sadek AM, Mahmoud RH. From parasite-induced immune activation to neuroinflammation and behavioral dysfunction: convergent mechanisms across protozoa and helminths: a review. Journal of Neuroinflammation. 2026;23:129. https://doi.org/10.1186/s12974-026-03804-4
- Abdoli A, Olfatifar M, Eslahi AV, et al. A systematic review and meta-analysis of protozoan parasite infections among patients with mental health disorders: an overlooked phenomenon. Gut Pathogens. 2024;16:7. https://doi.org/10.1186/s13099-024-00602-2
- Daré LO, Bruand PE, Gérard D, et al. Associations of mental disorders and neurotropic parasitic diseases: a meta-analysis in developing and emerging countries. BMC Public Health. 2019;19:1645. https://doi.org/10.1186/s12889-019-7933-4
- Ssemata AS, Nakitende AJ, Kizito S, et al. Association of severe malaria with cognitive and behavioural outcomes in low- and middle-income countries: a meta-analysis and systematic review. Malaria Journal. 2023;22:227. https://doi.org/10.1186/s12936-023-04653-9
- Hu A, Liu D, Xie H, et al. Depression in the schistosomiasis japonica population based on the PHQ-9 scale: a cross-sectional survey from Jiangxi Province, China. Scientific Reports. 2024;14:24323. https://doi.org/10.1038/s41598-024-74510-5
- Lee YL, Hu HY, Yen CM, et al. Pinworm infections associated with risk of psychiatric disorders: a nationwide cohort study in Taiwan. Comprehensive Psychiatry. 2019;93:14-19. https://doi.org/10.1016/j.comppsych.2019.02.002
Leave a Reply