⏱ 1 min read
A 2026 AB10015 post-hoc preprint reported 42.3% 5-year survival from amyotrophic lateral sclerosis symptom onset among patients originally assigned to masitinib 4.5 mg/kg/day with riluzole. The number is large for ALS, but the long-term comparison is historical and modeled rather than randomized placebo follow-up.1
Research Highlights
- 42.3% reached 5 years from onset: Ludolph et al. reported 55 of 130 patients surviving at least 5 years after ALS symptom onset in the masitinib 4.5 mg/kg/day arm.1
- Slower-progressing patients had higher survival than the full masitinib arm: 5-year survival rose to 50.0% in the AB10015 primary efficacy population with baseline ΔFS <1.1 points/month and 52.9% in the subgroup without complete loss of ALSFRS-R function.1
- ENCALS predicted much shorter survival: among 55 long-term survivors, observed median survival was 121 months vs. 42 months predicted by the ENCALS model, a 79-month residual median survival gap.1,4
- Function remained mixed, not uniformly preserved: 49.1% of the 55 long-term survivors had no permanent ventilation, gastrostomy, tracheostomy, or wheelchair dependence by the follow-up cutoff.1
- Evidence strength stays provisional: the analysis was a sponsor-involved 2026 medRxiv preprint without long-term randomized placebo follow-up, so the signal is hypothesis-strengthening rather than practice-changing.1
Amyotrophic lateral sclerosis (ALS) is a motor-neuron disease in which progressive loss of upper and lower motor neurons causes weakness, respiratory failure, and death. Median survival is often measured in years, not decades, so any 5-year survival signal deserves a careful read.
Masitinib is an oral tyrosine kinase inhibitor, meaning it blocks signaling enzymes that help immune and inflammatory cells activate. In ALS, the proposed rationale is not direct motor-neuron replacement; it is dampening microglial and mast-cell activity that may accelerate motor-neuron injury.
42.3% 5-Year Survival Is the Signal, Not the Proof
Ludolph et al. analyzed long-term survival in the masitinib 4.5 mg/kg/day arm of AB10015, an international randomized trial that originally tested masitinib added to riluzole in ALS.1,2 Riluzole is the long-standing first-line ALS drug; its survival effect is real but modest, which is why add-on therapies keep being tested.5
The headline number was 42.3%: 55 of 130 patients originally assigned to masitinib 4.5 mg/kg/day were alive at least 5 years after symptom onset. In patients with baseline ΔFS <1.1 points/month, the prespecified AB10015 primary efficacy population, 53 of 106 patients reached 5 years, or 50.0%.
ΔFS is the ALSFRS-R progression rate from symptom onset to baseline. Plain English: it estimates how quickly function had already been falling before trial entry. A lower ΔFS means slower early decline, so a higher survival rate in that group is clinically plausible even before drug effect is considered.
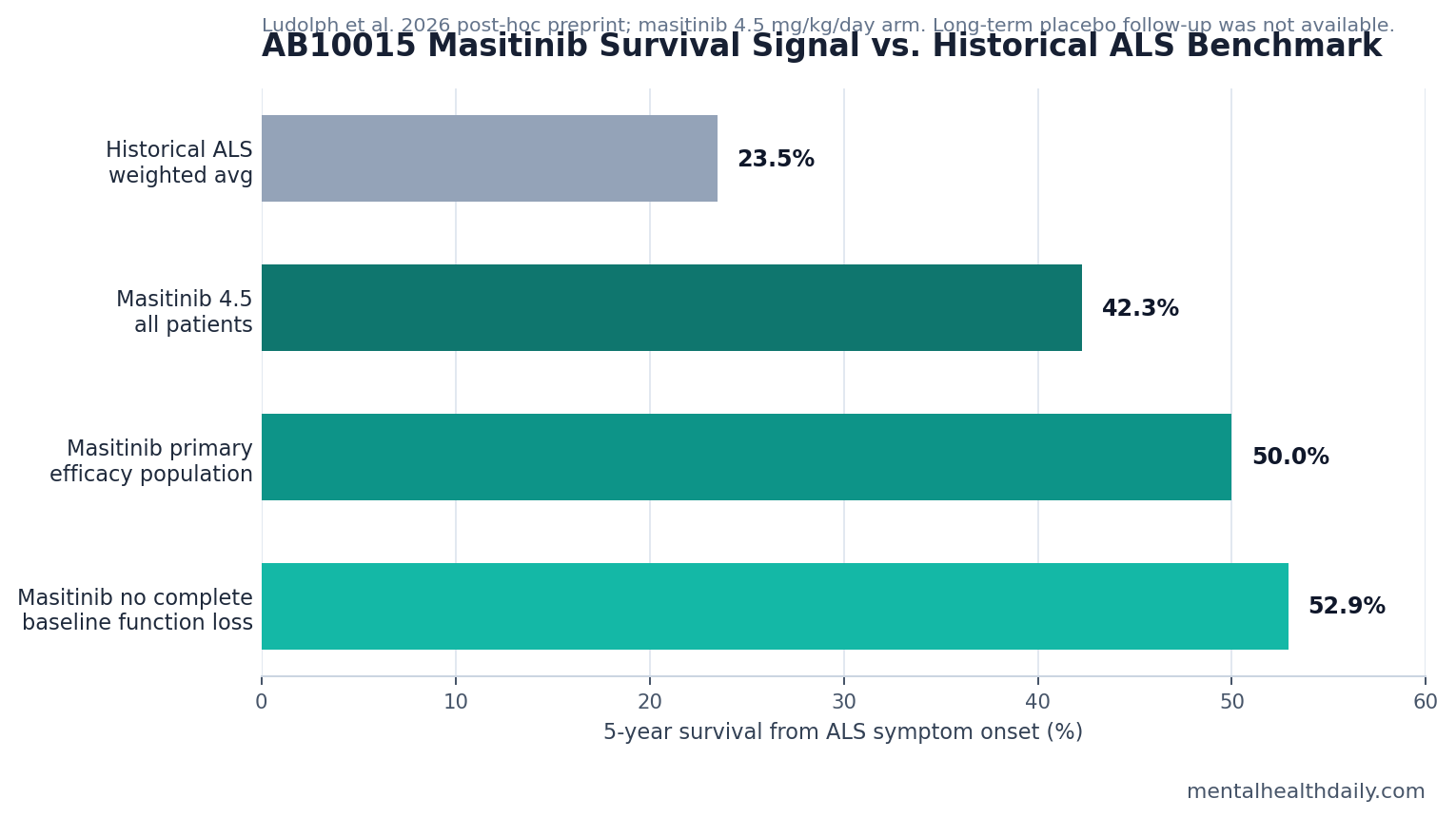
- All masitinib 4.5 mg/kg/day patients: 42.3% 5-year survival from symptom onset.
- Primary efficacy population: 50.0% 5-year survival when baseline ΔFS was <1.1 points/month.
- No complete baseline functional loss: 52.9% 5-year survival when every ALSFRS-R item was at least 1 at baseline.
- Historical benchmark in the paper: 23.5% weighted average 5-year ALS survival across cited cohorts.
Those are not small differences. The calibration is that the long-term comparison did not preserve randomized placebo follow-up across the same time horizon. After AB10015 ended, follow-up centered on patients continuing masitinib through compassionate or open-label access. That makes the result clinically interesting and methodologically vulnerable at the same time.
ENCALS Predicted 42 Months, While Observed Median Survival Was 121 Months
ENCALS is a personalized ALS survival prediction model that combines clinical and biological prognostic factors, including age at onset, diagnostic delay, site of onset, ALSFRS-R slope, respiratory function, and other variables.4 Ludolph et al. used it as a modeled comparator for the 55 masitinib-treated patients who had already survived at least 5 years.
For those long-term survivors, observed Kaplan-Meier median overall survival from symptom onset was 121 months, with a 95% confidence interval of 97 months to not reached. ENCALS-predicted median survival was 42 months, with a 95% confidence interval of 36 to 44 months. The residual median survival gap was 79 months, with p <0.0001.1
Another way to read the same comparison: 51 of 55 long-term survivors, or 92.7%, lived longer than their ENCALS prediction. Only 1 of 55 lived less than predicted, and 3 of 55 were within ±10% of predicted survival.
Model-comparison caveat: ENCALS predicts a composite survival outcome that includes death, tracheostomy, or near-continuous noninvasive ventilation. The 2026 masitinib analysis defined observed overall survival as time from symptom onset to death. That endpoint mismatch can inflate the apparent separation between observed and predicted survival if disability events occur before death.
Half of Long-Term Survivors Avoided Major Mechanical Assistance
Survival without context can mislead in ALS. Extending life while shifting patients into prolonged ventilatory dependence would be a different claim from extending survival with preserved functional independence.
Ludolph et al. did not collect formal quality-of-life questionnaires across the entire long-term window. Instead, they used a surrogate: no permanent ventilation, no gastrostomy, no tracheostomy, and no wheelchair dependence. By that definition, 27 of 55 long-term survivors, or 49.1%, maintained “satisfactory QoL.” The same 49.1% proportion appeared in the primary efficacy population, and the subgroup without complete baseline functional loss reached 55.6%.1
Clinical translation: the finding is not “patients lived longer with normal function.” It is narrower: about half of the long-term survivors had not crossed the paper’s major mechanical-assistance threshold by the cutoff. That still matters, but it should not be read as preserved speech, swallowing, walking, hand function, or daily independence across all domains.
Fast Progressors and Complete Baseline Functional Loss Were Less Represented
Table 3 is where the survival story becomes more selective. Fast progressors were 18.0% of the overall masitinib cohort but only 3.6% of the long-term survivor group. Patients with very severe baseline ALS, defined as a score of 0 on at least 1 ALSFRS-R item, were 25.0% of the overall cohort and 16.4% of long-term survivors.1
Slow progressors moved in the other direction: 18.0% of the overall cohort vs. 30.9% of long-term survivors. Moderate baseline severity was also more common among long-term survivors, at 50.9% vs. 39.1% in the overall masitinib cohort.
Patient-selection signal: masitinib looked more plausible before rapid decline or complete functional loss had already emerged. That matches the proposed mechanism. A drug designed to reduce inflammatory acceleration should be expected to slow ongoing damage, not rebuild motor neurons that are already lost.
Masitinib Fits the Immune-Glial ALS Hypothesis
Microglia are immune-like cells inside the central nervous system. In ALS, activated microglia can release inflammatory signals around vulnerable motor neurons. Mast cells are peripheral immune cells that can amplify inflammatory signaling and interact with nerve, vascular, and glial compartments.
Masitinib targets kinases linked to these cells, including CSF1R-related microglial signaling and KIT/LYN/FYN-linked mast-cell biology. The 2026 preprint argues that long-term survivors across several baseline prognostic groups may represent a subgroup whose ALS progression is especially driven by microglial or mast-cell activity.1
The mechanism is plausible enough to test. It is not proven by the long-term survivor analysis. The analysis selected patients who had already survived at least 5 years, compared them partly with historical and modeled expectations, and came from a trial program with sponsor involvement.
Biomarker implication: a future masitinib claim would be much stronger if a prespecified blood or cerebrospinal-fluid marker identified patients whose inflammatory biology predicts response before treatment. Without that, the field is left with a large survival signal and a patient-selection hypothesis, not a practical responder test.
Why This Does Not Settle Masitinib for ALS
The strongest version of the masitinib case is not that every caveat cancels the survival signal. A 42.3% 5-year survival rate, a 50.0% rate in the primary efficacy population, and a 79-month modeled median survival gap are too large to dismiss as ordinary noise.
The strongest skeptical reading is also straightforward: post-hoc long-term survival, missing long-term placebo follow-up, compassionate-use continuation, endpoint mismatch with ENCALS, sponsor involvement, and preprint status all push against treating the result as definitive.
- What the analysis can support: masitinib deserves continued prospective testing in selected ALS populations, especially earlier or slower-progressing disease.
- What it cannot support yet: a claim that masitinib has proven broad ALS survival benefit in routine practice.
- What would change the evidence level: randomized survival follow-up, prespecified responder biomarkers, and replication outside the sponsor-controlled analysis chain.
Optimal interpretation: the AB10015 long-term survivor analysis strengthens the case for masitinib as an ALS subgroup therapy. It does not remove the need for prospective confirmation.
Questions About Masitinib and ALS Survival
Does this prove masitinib extends ALS survival?
No. It reports a large survival signal in a post-hoc long-term analysis, but the decisive comparison was not long-term randomized placebo follow-up. The result is strong enough to justify further testing, not strong enough to settle clinical use.
Which ALS patients looked most likely to fit the signal?
The signal looked strongest in patients with slower baseline progression and no complete loss of function on any ALSFRS-R item at baseline. Fast progressors were sharply underrepresented among long-term survivors.
Why compare against ENCALS instead of only historical cohorts?
Historical cohorts give broad context, but ALS prognosis varies by age, respiratory function, site of onset, diagnostic delay, and early functional slope. ENCALS tries to account for those factors at the patient level. The limitation is that modeled survival is still not the same as a live randomized placebo group.
What would make the masitinib claim more convincing?
A prospective trial that preserves survival follow-up across treatment and control arms would matter most. A validated biomarker showing that masitinib responders have a specific microglial or mast-cell inflammatory profile would also make patient selection more credible.
References
- Ludolph AC, Heiman-Patterson T, Mora JS, Rodriguez G, Bohorquez Morera N, Vermersch P, et al. Evaluation of long-term amyotrophic lateral sclerosis survivors treated with masitinib in study AB10015. medRxiv. 2026. https://doi.org/10.64898/2026.04.10.26350104
- Mora JS, Genge A, Chio A, Estol CJ, Chaverri D, Hernandez M, et al. Masitinib as an add-on therapy to riluzole in patients with amyotrophic lateral sclerosis: a randomized clinical trial. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration. 2020;21(1-2):5-14. https://doi.org/10.1080/21678421.2019.1632346
- Mora JS, Bradley WG, Chaverri D, Hernandez M, Reyes E, Wang YC, et al. Long-term survival analysis of masitinib in amyotrophic lateral sclerosis. Therapeutic Advances in Neurological Disorders. 2021;14:17562864211030365. https://doi.org/10.1177/17562864211030365
- Westeneng HJ, Debray TPA, Visser AE, van Eijk RPA, Rooney JPK, Calvo A, et al. Prognosis for patients with amyotrophic lateral sclerosis: development and validation of a personalised prediction model. Lancet Neurology. 2018;17(5):423-433. https://doi.org/10.1016/S1474-4422(18)30089-9
- Miller RG, Mitchell JD, Moore DH. Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND). Cochrane Database of Systematic Reviews. 2012;2012(3):CD001447. https://doi.org/10.1002/14651858.CD001447.pub3
- Brooks BR, Berry JD, Ciepielewska M, Liu Y, Zambrano GS, Zhang J, et al. Intravenous edaravone treatment in ALS and survival: an exploratory, retrospective, administrative claims analysis. EClinicalMedicine. 2022;52:101590. https://doi.org/10.1016/j.eclinm.2022.101590
Leave a Reply