
⏱ 8 min read
A 40-person pilot trial found depression remission in 69% of adults who did 30 minutes of moderate exercise before individual CBT, compared with 33% of adults who did a calming pre-CBT activity.1 Compared with a broad “exercise boosts therapy” claim, acute exercise is a plausible priming step; the alliance and activation mechanisms still need a larger trial.
Research Highlights
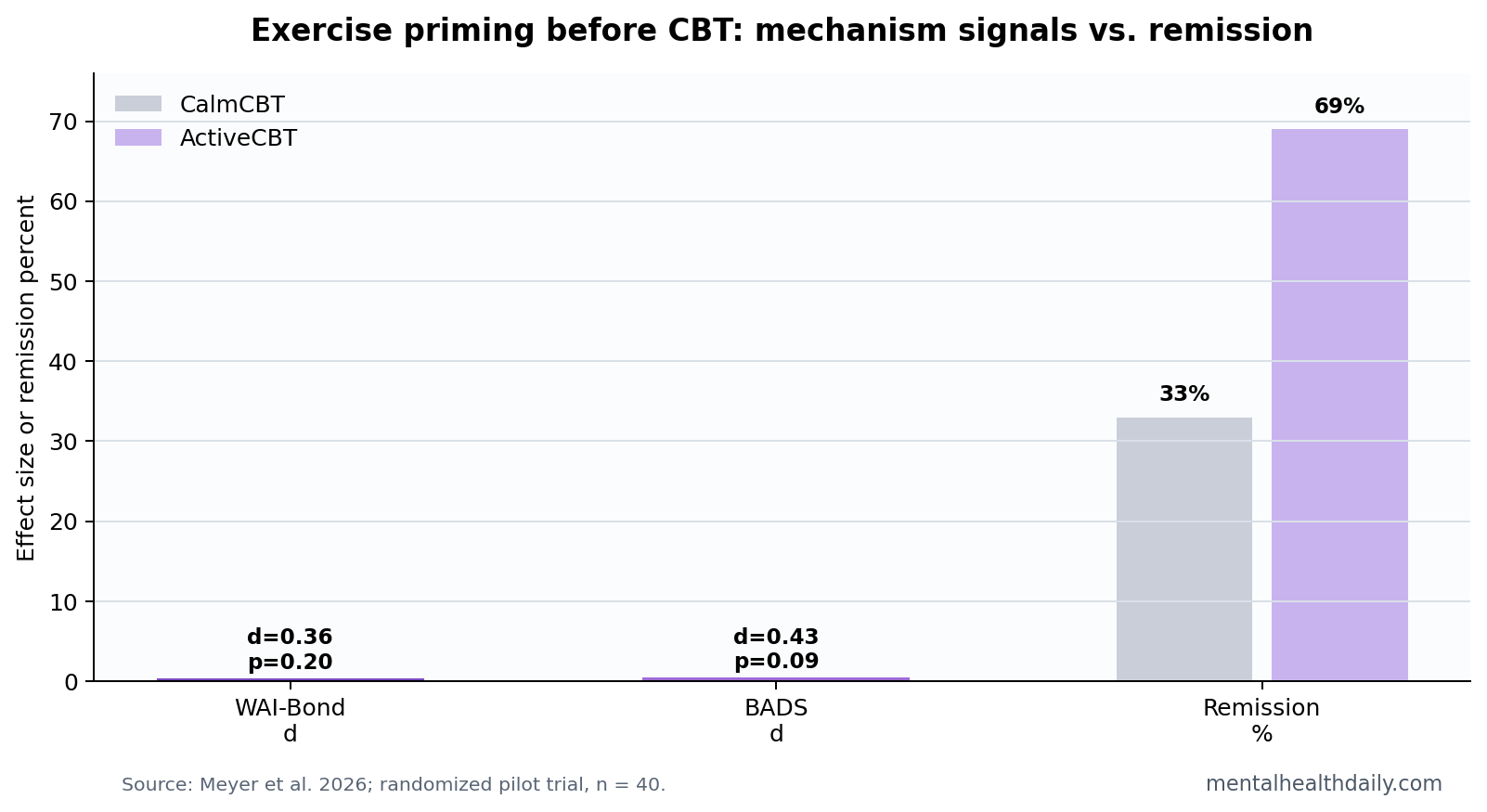
- Remission favored exercise priming: 69% of ActiveCBT participants remitted vs. 33% of CalmCBT participants, p < 0.05, in a 40-person pilot trial.1
- Mechanism effects leaned positive: WAI-Bond favored ActiveCBT at d = 0.36, 95% CI −0.19 to 0.90, p = 0.20, and BADS favored ActiveCBT at d = 0.43, 95% CI −0.07 to 0.94, p = 0.09.1
- Response was less distinctive: remission separated the groups more clearly than 50% symptom response, which looked similar across arms.1
- Exercise evidence is already broad: a 2024 network meta-analysis found antidepressant effects across multiple exercise formats, but it did not test pre-session exercise as a psychotherapy primer.3
- Clinical use remains provisional: n = 40 is enough for a target-engagement signal, not enough for a practice-changing sequencing rule.1
Exercise priming means using a short bout of activity immediately before psychotherapy to change the state in which a patient enters the session. The proposed pathway is simple: moderate exercise can increase arousal, improve affect, make approach behavior easier, and potentially make the first minutes of CBT less avoidant.
Cognitive behavioral therapy (CBT) is a structured psychotherapy that helps patients identify patterns of thought and behavior that maintain symptoms. In depression, CBT often depends on behavioral activation: helping patients re-enter rewarding or meaningful activity instead of waiting for motivation to return.
30 Minutes of Exercise Before CBT Targeted Alliance and Activation
Meyer et al. randomized 40 adults with DSM-5 major depressive disorder to 8 weeks of individual CBT. ActiveCBT participants did 30 minutes of moderate exercise before therapy sessions; CalmCBT participants did a calming activity before the same therapy structure.1
The trial was designed as a target-engagement study. Instead of only asking whether symptoms changed, researchers asked whether the pre-session exercise dose changed 2 therapy-relevant mechanisms:
- Therapeutic bond: measured with the Working Alliance Inventory Bond subscale, which captures the felt collaborative connection between patient and therapist.
- Behavioral activation: measured with the Behavioral Activation for Depression Scale, which captures approach behavior, avoidance, and engagement with rewarding activity.
Both mechanism measures leaned toward ActiveCBT. Neither effect was statistically confirmed. That distinction is the central calibration: the data point in the expected direction, but the confidence intervals still include small or absent effects.
69% Remission Was Stronger Than the Mechanism Readout
Remission on the interviewer-administered Hamilton Rating Scale for Depression separated the groups sharply: 69% in ActiveCBT vs. 33% in CalmCBT, p < 0.05.1 That is the most reader-relevant number in the trial.
Symptom response, defined as at least 50% reduction, did not separate the arms as clearly. A remission advantage without a similarly clean response advantage can happen in a small sample when several participants cluster near the remission threshold. It still deserves attention, but it should not be inflated into a definitive clinical effect.
Evidence-strength note: this was a pilot randomized trial. It can tell researchers whether the protocol is feasible and whether target mechanisms move in the expected direction. It cannot prove that exercise before CBT reliably doubles remission in routine care.
Exercise and CBT Evidence Support the Idea, Not the Exact Sequence
Adjacent evidence makes the priming hypothesis plausible. Psychotherapy for adult depression has broad evidence, with CBT among the main supported approaches.2 Exercise also has antidepressant evidence across many trial formats, though effects vary by modality, intensity, comparator, and adherence.3
The Meyer trial asked a narrower question than either literature usually answers. It did not compare exercise vs. CBT. It tested whether exercise could change the patient state immediately before CBT enough to improve therapy-relevant processes.
Behavioral activation is a reasonable target for that question. Activation models treat depression partly as a loop of avoidance, low reward, withdrawal, and reduced contact with reinforcing experiences.4 If exercise temporarily makes approach behavior easier, a CBT session right afterward might be a better moment to plan, rehearse, or commit to behavioral activation tasks.
Practical Use Should Stay Low-Risk and Optional
For now, the useful clinical version is modest: for patients who already tolerate exercise, a brief moderate session before therapy may be worth testing as a personal routine. The trial does not support requiring exercise as a gate to CBT, blaming patients who cannot exercise, or treating activity as a replacement for therapy.
Implementation should preserve choice:
- Medical limits: screen for cardiovascular, orthopedic, eating-disorder, and fatigue-related risks before recommending pre-session exertion.
- Adherence: a priming routine that makes therapy harder to attend is counterproductive.
- Alternative primers: light walking, stretching, sunlight exposure, or brief activation planning may be safer for some patients.
Why Remission Can Move Before the Mechanism Is Proven
A small trial can produce a visible clinical split before it can explain the split. That is especially true when the mechanism measure is noisy, the treatment dose is brief, and the sample size is only 40.
WAI-Bond and BADS were reasonable target measures, but neither is a direct recording of what happens inside a therapy session.
Working alliance is partly a relationship measure, partly a task-and-goal agreement measure, and partly a patient-state measure. A person who has just exercised may feel more awake, more cooperative, or more hopeful during a session, but that does not guarantee a sustained alliance change large enough for a questionnaire to catch.
Behavioral activation is also broader than a single post-exercise window. The BADS asks about patterns over the preceding week. A 30-minute pre-session exercise dose could make the therapy hour more productive without immediately changing the whole week’s avoidance, routine, reward exposure, or follow-through.
A stronger trial would measure both levels at once: immediate session state and week-level behavior. That would separate a short-lived priming effect from a durable activation effect, and it would show whether remission follows better therapy engagement, more completed homework, or a nonspecific expectation boost.
It should also track adverse friction: missed sessions, soreness, embarrassment, fatigue, and whether exercise made therapy easier or harder to attend.
Comparator choice: the calming activity was a reasonable control because it gave the comparison group a pre-therapy ritual. A future trial should keep that design logic. If exercise is compared with no added activity, the study cannot separate movement-specific priming from attention, expectancy, schedule structure, or the psychological effect of doing something active before therapy.
The exercise dose also needs practical testing. A 30-minute block before every CBT session may be easy in a research protocol and difficult in ordinary care, especially when appointments happen before work, during lunch, or by telehealth. A shorter walk, stairs session, stationary bike option, or home-based warm-up may preserve the state-change idea with less attendance friction.
Therapists would also need a way to adjust the primer when sleep, pain, panic, or medication side effects make exertion a poor fit that day.
This is why the remission signal should be neither dismissed nor oversold. If the next trial finds the same remission direction and shows repeated activation gains between sessions, the case for exercise priming becomes stronger. If remission fails to replicate, the current result becomes a useful pilot artifact rather than a treatment rule.
Sequencing May Matter More Than Exercise Type
The broader exercise-for-depression literature often asks which exercise modality works best. That question is useful for prescribing activity. The Meyer trial asked a different question: whether activity immediately before therapy changes the treatment context.
That sequencing question matters because depression often blocks action at the moment action is needed. A patient may understand CBT homework, agree with the plan, and still leave the office without enough behavioral momentum to start. If moderate exercise increases energy, reward sensitivity, or willingness to approach effort for a short window, pairing it with CBT could be more useful than placing exercise elsewhere in the week.
Still, the safest implementation would be individualized. Some patients become calmer after exercise. Others become exhausted, self-conscious, sweaty, dysregulated, or pain-limited. A pre-CBT primer should improve the therapy hour, not turn the appointment into a second performance test.
Questions About Exercise Before CBT for Depression
Does this mean exercise should replace CBT?
No. The trial tested exercise before CBT, not exercise instead of CBT. The intervention was a sequencing add-on to structured therapy.
Was the mechanism proven?
No. WAI-Bond and BADS both favored ActiveCBT, but their p-values were 0.20 and 0.09. Those values are compatible with a real signal, but not with a confirmed mechanism.
Who might try this first?
The best near-term candidates are adults who already find moderate activity tolerable and who enter therapy sessions withdrawn, flat, or avoidant. Patients with medical risks or exercise intolerance need a different activation strategy.
What study would clarify the result?
A larger trial should test the same pre-session exercise dose, preserve blinded symptom assessment, measure alliance and activation repeatedly, and pre-specify remission as a clinical endpoint rather than treating it as a pilot signal.
References
- Meyer JD, et al. Exercise priming to enhance therapeutic bond and behavioral activation in CBT for MDD: a randomized controlled target-engagement trial with remission signal. Journal of Affective Disorders. 2026;405:121606. https://doi.org/10.1016/j.jad.2026.121606
- Cuijpers P, et al. Psychotherapies for depression in adults: a network meta-analysis covering efficacy and acceptability. World Psychiatry. 2020;19:92-107. https://doi.org/10.1002/wps.20701
- Noetel M, et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2024;384:e075847. https://doi.org/10.1136/bmj-2023-075847
- Manos RC, Kanter JW, Busch AM. A critical review of assessment strategies to measure the behavioral activation model of depression. Clinical Psychology Review. 2010;30:547-561. https://doi.org/10.1016/j.cpr.2010.03.008
Leave a Reply