⏱ 9 min read
The link between psychological stress and chronic inflammation is well-documented — what’s been less clear is which specific inflammatory proteins move with anxiety in real-world community samples. A 2026 analysis from Loomans-Kropp et al. measured a 33-marker panel in 190 minoritized and medically underserved adults from the Cancer Disparities Research Network and identified three biomarkers (gp130, MMP-1, APRIL) significantly associated with anxiety after multivariable adjustment.1
Research Highlights
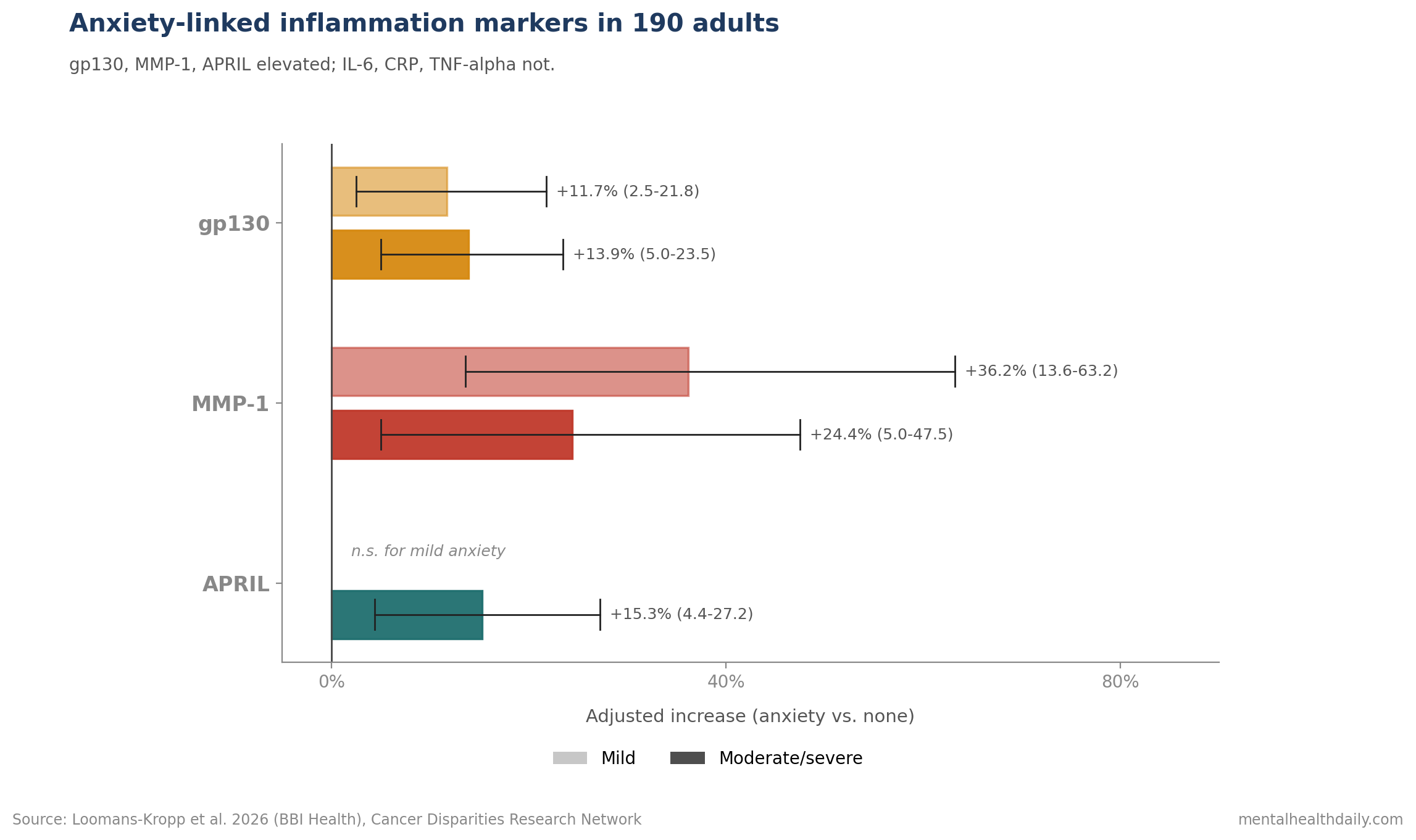
- gp130 elevation at 2 anxiety levels: mild anxiety was linked to an 11.7% higher geometric mean (95% CI 2.5–21.8%), while moderate/severe anxiety was linked to a 13.9% higher geometric mean (95% CI 5.0–23.5%) after multivariable adjustment.1
- MMP-1 was the largest signal: mild anxiety was associated with a 36.2% higher geometric mean (95% CI 13.6–63.2%), and moderate/severe anxiety with a 24.4% higher geometric mean (95% CI 5.0–47.5%).1
- APRIL tracked higher anxiety severity: moderate/severe anxiety was associated with a 15.3% higher geometric mean (95% CI 4.4–27.2%) vs. none, while mild anxiety did not show the same significant signal.1
- IL-6 was not the signal: the 33-marker panel pointed to IL-6-related receptors (gp130) and matrix-remodeling enzymes (MMP-1), not the conventional IL-6 / CRP / TNFα biomarkers that dominate the literature.1
- 190 underserved adults broadened the evidence: participants were 40–74 years old in medically underserved areas, with low literacy, low income, or uninsured status, extending biomarker work beyond the usual higher-resource cohorts.1
Roughly 35% of US adults have systemic chronic inflammation, and the bidirectional relationship between psychological state and immune signaling has been mapped for at least two decades.2
The contribution is biomarker specificity in a population the inflammation literature has rarely studied at this depth.
Traditional inflammation-anxiety research often focuses on a small set of cytokines (IL-6, CRP, TNFα). The Loomans-Kropp panel let the data choose, and the clearest markers were not the usual suspects.
190 Underserved Adults Received a 33-Marker Inflammation Panel
The Cancer Disparities Research Network (CDRN) is a National Cancer Institute regional unit focused on building cancer health disparities research in minoritized and underserved populations.1
The cohort:
- n = 190 adults, ages 40–74, recruited from 4 US institutions (University of Illinois Chicago, Tufts, Ohio State, Fox Chase) between January 2015 and April 2017.
- Eligibility required living in an Appalachian county or self-identifying as White, African American, Hispanic, or Asian, plus at least one of: medically underserved area, low literacy, low income (under $11,670 individual / $23,850 family of four), or uninsured/Medicaid status.
- Exclusions: nursing-home residence, pregnancy, or prior invasive cancer.
Each participant completed a baseline survey covering self-reported anxiety, fatigue, distress, and quality of life on 0–10 Likert scales, and gave a blood sample.
Plasma biomarkers were measured with a customized 33-analyte Luminex panel including: gp130 (an IL-6 family receptor), APRIL (a proliferation-inducing ligand), MMP-1 and MMP-3 (matrix metalloproteinases), TNFRI/TNFRII (tumor necrosis factor receptors), IL-6, IL-8, IL-10, IL-15, TNFα, adiponectin, and many others.
Anxiety responses were collapsed into three categories: none, mild, and moderate/severe. Multivariable linear regressions modeled log-transformed biomarker concentrations on anxiety category, with stepwise adjustment for demographics, lifestyle, and comorbidities.
Three Markers Stood Out: gp130, MMP-1, APRIL
gp130 is glycoprotein 130, the signal-transducing subunit of the IL-6 receptor family.1 Soluble gp130 in plasma helps regulate trans-signaling by IL-6 and related cytokines.
The interesting wrinkle: IL-6 itself did not associate with anxiety in this cohort, but gp130 did. The interpretation is that the regulatory layer of IL-6 family signaling, not the cytokine itself, may be the more sensitive readout in this population.
MMP-1 (matrix metalloproteinase-1) is a zinc-dependent endopeptidase that proteolytically processes the extracellular matrix.1 Beyond its tissue-remodeling role, MMP-1 has documented connections to neuronal plasticity in the brain, and elevated levels have been linked to obesity, cardiovascular disease, and psychological stress.
The MMP-1 signal in this cohort was the largest in absolute terms: 36.2% higher in mild anxiety and 24.4% higher in moderate/severe anxiety vs. no anxiety.
APRIL (a proliferation-inducing ligand) is a TNF-family cytokine involved in B-cell and plasma-cell biology.1 Its association with anxiety was new in this analysis and dose-dependent — only moderate/severe anxiety showed elevation, with a 15.3% higher geometric mean.
The dose-response pattern across the three markers is informative. gp130 and MMP-1 elevated at both anxiety levels; APRIL only at higher severity. Three markers, three slightly different sensitivity profiles to anxiety severity.
What the Conventional Cytokines Did Not Show
The familiar inflammation-anxiety markers in the broader literature — CRP, IL-6, TNFα, IL-1β — have been linked to depression and anxiety in dozens of studies.3
In this specific cohort, those associations did not hold up after adjustment.
IL-6: not significantly associated with anxiety in any adjusted model.1
TNFα / TNFRI / TNFRII: not significant after adjustment.
Adiponectin: significant in Model 1 (basic adjustment) but lost significance in Model 2 after race was added (p = 0.21). This suggests racial/ethnic confounding rather than an independent anxiety-adiponectin link in this sample.
Two reasonable explanations for the IL-6 / CRP / TNFα null fit the data.
First, sample size. n = 190 is modest for a 33-marker panel, and the conventional cytokines may have effect sizes that require larger cohorts to detect.
Second, population specificity. The CDRN cohort consists of minoritized, underserved adults with documented higher chronic-stress exposure than typical inflammation-anxiety study samples. Chronic activation may shift which markers are most sensitive to additional anxiety-related variance.
gp130, MMP-1, and APRIL Point to 3 Immune-Stress Pathways
The three positive markers point toward different aspects of immune-stress signaling.
gp130 and the IL-6 trans-signaling system. IL-6 has two signaling modes — classical (through membrane-bound IL-6R, mostly anti-inflammatory) and trans (through soluble IL-6R, mostly pro-inflammatory). Soluble gp130 binds the IL-6/sIL-6R complex and can buffer the trans-signaling pathway. Elevated gp130 in anxiety might reflect a compensatory upregulation of this regulatory layer in chronically stressed individuals.
MMP-1 and matrix remodeling. Beyond tissue physiology, MMP-1 is expressed in the brain and is associated with neuronal plasticity. Astrocyte-derived MMP-1 has been shown to modulate anxiety and social behavior in animal models.1 Whether peripheral MMP-1 reflects central remodeling activity is an open question; the elevation in anxiety here is consistent with a stress-immune-CNS axis hypothesis.
APRIL and adaptive immunity. APRIL’s role in B-cell biology connects anxiety to humoral immunity. The dose-response pattern (only severe anxiety elevates APRIL) suggests this marker may track sustained immune activation rather than transient stress response.
None of these mechanisms is settled. The Loomans-Kropp paper is hypothesis-generating for follow-up biomarker validation studies.
No Clinical Anxiety Test or Anti-Inflammatory Shortcut Follows Yet
- Psychological-immune coupling is measurable. Anxiety in this cohort tracked with peripheral biomarker changes, supporting the broader literature on stress-related immune signaling.3
- Don’t expect IL-6 or CRP to be the only relevant markers. The most-cited inflammation-anxiety biomarkers may be less sensitive than less-publicized ones (gp130, MMP-1, APRIL) in some populations.
- Health-disparity context matters for biomarker research. Generalizing findings from predominantly White, middle-class research cohorts to minoritized and underserved populations may miss real associations and obscure effective targets.
- This is not a clinical test. gp130, MMP-1, and APRIL panels are research tools. Patients with anxiety should not order these labs hoping to track their disorder. Clinical anxiety management still runs through symptom-based assessment and evidence-based psychotherapy or pharmacotherapy.
- Anti-inflammatory adjuncts are an active research area. Cytokine-targeted therapies (anti-IL-6, anti-TNF) have shown some signal in subsets of treatment-resistant depression. Whether parallel approaches benefit anxiety is unclear.
Cross-Sectional 190-Person Biomarker Data Cannot Prove Causality
It is cross-sectional. Anxiety and biomarkers were measured at a single time point. The analysis cannot distinguish whether anxiety drives the biomarker elevation, the biomarker pattern drives anxiety, or both share an upstream cause (chronic stress, early-life adversity, social determinants).
Anxiety was self-reported and categorical. Validated anxiety instruments (GAD-7, BAI) were not used. The 0–10 Likert collapsed to three categories may miss finer-grained dose-response patterns.
Sample size is modest for the marker panel. 33 markers in 190 participants raises multiple-comparison concerns. The authors report only the markers that were not correlated with each other and that survived adjustment, which mitigates but does not eliminate false-positive risk.
The cohort was specifically minoritized and underserved. Generalizability to other populations is not established; the conventional-cytokine null in this analysis may not replicate in higher-resource samples.
Causal direction is untested. Whether reducing anxiety would lower gp130 / MMP-1 / APRIL, or whether modulating these biomarkers would reduce anxiety, is not addressable in this cross-sectional design.
Questions About Anxiety, Inflammation, and Specific Biomarkers
Is there an inflammation test for anxiety?
No. gp130, MMP-1, and APRIL are research markers, not clinical diagnostics for anxiety disorders.1
Anxiety diagnosis remains symptom-based, using validated instruments like the GAD-7 or clinical interview. The Loomans-Kropp findings inform mechanism research; they do not change diagnosis or treatment selection.
Why didn’t IL-6 show up if it’s the most-cited inflammation-anxiety marker?
Two plausible reasons. First, sample size: n = 190 is modest for detecting smaller effects, and IL-6 effects in inflammation-anxiety studies are typically modest. Second, population specificity: this cohort was minoritized and underserved with documented higher baseline chronic stress, where conventional markers may be less sensitive than markers further upstream or downstream in the signaling chain.1
Should I take anti-inflammatory drugs for anxiety?
The evidence does not yet support routine anti-inflammatory treatment for anxiety. Cytokine-targeted therapies (e.g., anti-IL-6) have shown signals in specific subsets of treatment-resistant depression, but parallel anxiety evidence is thin.3
Established anxiety treatments (CBT, SSRIs/SNRIs, exposure therapy) remain first-line.
Does this mean stress causes physical disease?
The evidence base supports that chronic stress and anxiety contribute to inflammation, which in turn contributes to risk for cardiovascular disease, metabolic disease, and possibly cancer.2
The Loomans-Kropp findings add specificity to that picture by identifying gp130, MMP-1, and APRIL as candidate intermediaries in the mind-body pathway.
What about depression and inflammation? Same biomarkers?
Partly overlapping. Depression has a stronger and more replicated link to IL-6, CRP, and TNFα in the inflammation literature. Whether gp130, MMP-1, and APRIL emerge for depression in similarly underserved cohorts is an open empirical question.3
References
- Chronic inflammation is associated with increased anxiety in the Cancer Disparities Research Network. Loomans-Kropp H et al. Brain, Behavior, & Immunity – Health. 2026;54:101233. doi:10.1016/j.bbih.2026.101233
- Chronic inflammation in the etiology of disease across the life span. Furman D et al. Nature Medicine. 2019;25(12):1822-1832. doi:10.1038/s41591-019-0675-0
- A meta-analysis of cytokines in major depression. Dowlati Y et al. Biological Psychiatry. 2010;67(5):446-457. doi:10.1016/j.biopsych.2009.09.033
- Stress, inflammation and the gut microbiota: implications for human health. Bailey MT & Coe CL. Brain, Behavior, and Immunity. 2015;47:1-3. doi:10.1016/j.bbi.2015.02.025
- Anti-inflammatory treatment for major depression: implications for inflammatory subtypes. Raison CL & Miller AH. Psychiatric Clinics of North America. 2013;36(1):283-298. doi:10.1016/j.psc.2012.12.005
Leave a Reply