
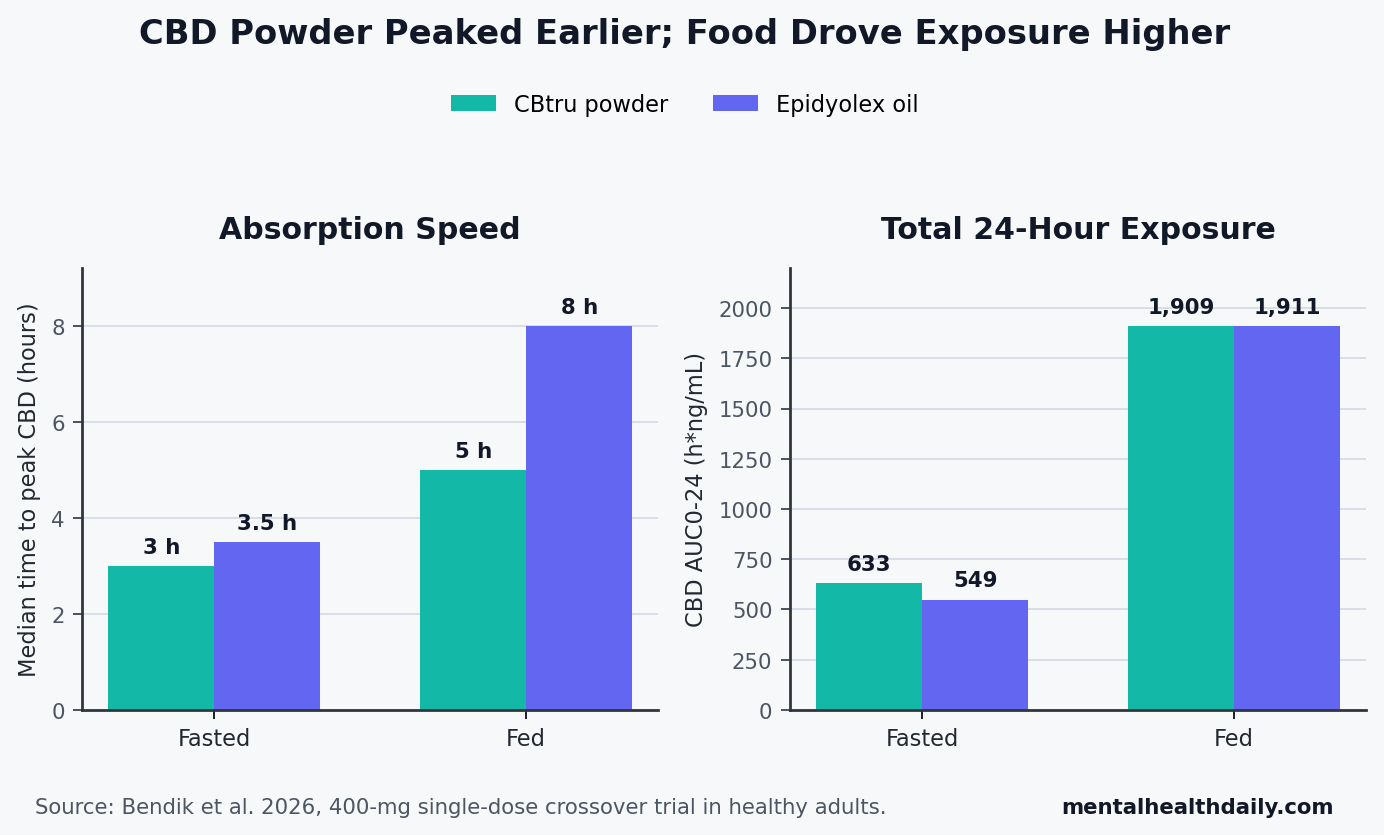
A 2026 Phase I crossover trial found that a 400-mg powdered cannabidiol formulation reached peak CBD faster than Epidyolex oil in healthy adults — 3 h vs. 3.5 h when fasted and 5 h vs. 8 h after a high-fat meal — but food still dominated the exposure story.1
Research Highlights
- Faster peak: CBtru powder reached median peak CBD concentration sooner than Epidyolex oil in both fasted dosing (3 h vs. 3.5 h; p = 0.015) and fed dosing (5 h vs. 8 h; p < 0.001).1
- Comparable fed exposure: after a high-fat meal, 24-hour CBD exposure was almost identical between CBtru and Epidyolex: 1909 vs. 1911 h*ng/mL, with no significant formulation difference.1
- Fasted metabolite signal: CBtru produced higher fasted exposure to 7-OH-CBD and 7-COOH-CBD, with AUC ratios of 149.2% and 158.4% vs. Epidyolex.1
- Food effect remained large: fed dosing raised CBD exposure about 3.0-fold with CBtru and 3.5-fold with Epidyolex, matching older CBD food-effect work.1,2
- Evidence limit: the trial measured pharmacokinetics and short-term tolerability in healthy adults, not seizure control, anxiety, sleep, pain, or psychiatric efficacy.1
Cannabidiol (CBD) is a non-intoxicating cannabis-derived compound used as a prescription antiseizure drug in purified form and marketed far more broadly for anxiety, sleep, pain, and inflammation. For oral CBD, clinical interpretation depends heavily on whether a swallowed dose produces predictable blood levels.
Pharmacokinetics means how a drug moves through the body: absorption, peak concentration, total exposure, metabolism, and clearance. For oral CBD, that machinery is unusually messy because CBD is highly fat-soluble, poorly water-soluble, and strongly affected by meals.
CBtru Powder Peaked Faster Than Epidyolex Oil
Bendik et al. randomized 32 healthy adults to receive a single 400-mg dose of CBtru, a powdered emulsion CBD capsule, and Epidyolex, the approved sesame-oil CBD oral solution. Each person was assigned to 4 treatment periods: CBtru fasted, Epidyolex fasted, CBtru fed, and Epidyolex fed, with at least 14 days of washout between doses.1
The main reader-facing result is about timing, not a proven clinical advantage. Time to maximum concentration (tmax) is the time it takes a drug to reach its measured peak blood level. CBtru reached peak CBD sooner than Epidyolex in both food states:
- Fasted dosing: CBtru reached median peak CBD at 3.0 h vs. 3.5 h with Epidyolex (p = 0.015).
- Fed dosing: CBtru reached median peak CBD at 5.0 h vs. 8.0 h with Epidyolex (p < 0.001).
- Metabolite timing: 7-OH-CBD, an active CBD metabolite, also peaked earlier with CBtru after the high-fat meal: 5.0 h vs. 12.0 h (p = 0.005).
Area under the curve (AUC) is total drug exposure over time. Faster peaking did not automatically mean much greater parent-CBD exposure.
Under fasted conditions, CBtru had numerically higher CBD AUC0-24 than Epidyolex (633 vs. 549 h*ng/mL), but the adjusted ratio did not reach statistical significance (115.3%; p = 0.204). CBD maximum concentration also leaned higher with CBtru (154.8 vs. 115.0 ng/mL), but that comparison was borderline rather than formally significant (p = 0.065).1
After the high-fat breakfast, the parent-CBD exposure comparison nearly disappeared. CBtru and Epidyolex produced almost the same CBD AUC0-24: 1909 vs. 1911 h*ng/mL, with an adjusted ratio of 99.3% (p = 0.946). The better-supported formulation claim is therefore narrower: CBtru shifted absorption earlier and may reduce variability, but it did not clearly beat Epidyolex on total fed-state CBD exposure.
Fasted Metabolite Exposure Favored the Powder Formulation
CBD exposure includes parent CBD and its metabolites, especially 7-OH-CBD (7-hydroxy-cannabidiol, an active metabolite) and 7-COOH-CBD (7-carboxy-cannabidiol, the major circulating inactive metabolite). Bendik et al. also combined parent CBD and metabolites into active drug exposure and total drug exposure measures.1
The strongest CBtru signal appeared in fasted metabolite exposure. Compared with Epidyolex, CBtru produced higher 24-hour exposure to 7-OH-CBD (149.2%; p < 0.001) and 7-COOH-CBD (158.4%; p < 0.001). Active drug exposure, defined as CBD plus 7-OH-CBD, was also higher (127.1%; p = 0.013), and total drug exposure was higher (154.5%; p < 0.001).
That result is pharmacologically interesting, but it should not be inflated into efficacy language. Higher metabolite exposure may matter for clinical effect, adverse effects, or drug interactions, but this trial did not test symptom outcomes. It also did not establish whether more 7-OH-CBD is better for any psychiatric or neurological indication.
Safety signal: both formulations were tolerated in this short study. The trial recorded mostly mild treatment-emergent adverse events, 1 moderate drowsiness event, and no serious or severe adverse events. Headache appeared in 18.8% of participants, loose stool and nausea each in 9.4%, and the lab-related adverse events were judged mild and unrelated to treatment.1
Food Still Changed CBD Exposure More Than Formulation Did
The fed-state protocol used a standardized high-fat, high-calorie breakfast: 800 to 1000 kcal, about 50% from fat, eaten within 30 min before CBD dosing. That design matters because CBD exposure is meal-sensitive.
Magnitude: in the 2026 trial, food raised CBD exposure more than the formulation swap did. Fed vs. fasted AUC0-24 rose 3.01-fold for CBtru and 3.50-fold for Epidyolex, both with p < 0.001. Maximum CBD concentration also rose substantially: 2.09-fold for CBtru and 2.25-fold for Epidyolex.1
Adjacent evidence: Taylor et al. previously tested highly purified CBD in healthy adults and reported a strong food effect, which is why modern CBD pharmacokinetic studies treat fed and fasted dosing as separate conditions rather than minor background details.2
Crockett et al. later showed that meal composition, whole milk, and alcohol could change CBD exposure and tolerability patterns, reinforcing that “take with food” is not a trivial instruction for CBD.3
Saals et al. added a newer CBD-rich extract result: a high-fat meal changed CBD bioavailability and biphasic absorption, meaning blood levels can show more than 1 peak as digestion, lymphatic transport, and later meals shape absorption.4 Bendik et al. discussed that double-peak pattern as one possible explanation for fed-state concentration profiles.
For readers, the practical interpretation is simple: a more efficient formulation may reduce some absorption variability, but inconsistent food timing can still produce large CBD exposure swings.
Self-Emulsifying CBD Work Points in the Same Direction
CBtru is not a generic CBD powder. It is an emulsion-based solid powder formulation, designed so CBD disperses into smaller droplets and interacts more efficiently with bile salts and intestinal lipids. That logic overlaps with self-emulsifying drug delivery systems (SNEDDS), which are formulations built to form fine oil-in-water dispersions in the gut.
Izgelov et al. compared synthetic CBD in sesame oil with a capsule-based self-emulsifying formulation in healthy volunteers. The broader pattern was similar to the Bendik trial: formulation engineering can make early absorption more uniform even when total exposure is not dramatically different.5
Bendik et al. reported lower geometric coefficients of variation with CBtru than Epidyolex for CBD AUC0-24 in both conditions: 70.0% vs. 80.8% when fasted and 35.1% vs. 54.4% when fed. For CBD peak concentration, variability was also lower with CBtru: 73.5% vs. 117.1% when fasted and 61.4% vs. 73.3% when fed.1
Clinical implication: lower variability could matter if future patient trials show that steadier CBD exposure improves tolerability, adherence, or therapeutic response. Until those trials exist, the claim remains a dosing-platform hypothesis.
The Trial Does Not Prove Better CBD Treatment
The sponsor-developed formulation performed well on several pharmacokinetic endpoints, but the study design was intentionally early-stage. It used a single 400-mg dose in healthy adults, followed blood levels for 24 h, and measured short-term safety. That is the correct design for an initial formulation comparison, but it cannot answer patient-outcome questions.
Evidence-strength note: this trial supports claims about single-dose absorption speed, exposure, metabolite profiles, variability, and acute tolerability. It cannot show better seizure control, better anxiety reduction, better sleep, less pain, fewer long-term adverse effects, or safer chronic polypharmacy.
Several limits should stay visible:
- Population: healthy adults are cleaner for pharmacokinetic testing, but they are not children with drug-resistant epilepsy, anxious patients, chronic pain patients, or older adults taking multiple interacting drugs.
- Dosing: 1 dose cannot establish steady-state levels, accumulation, dose proportionality, or long-term tolerability.
- Sampling: 24-hour sampling captured most exposure but did not fully define terminal elimination for some analytes.
- Sponsor context: the trial was funded by the company developing CBtru, so replication in independent patient trials would carry real value.
The calibrated read is favorable but bounded. CBtru looks like a plausible oral CBD delivery improvement, especially for faster absorption and reduced variability. It is not yet evidence that a CBD powder formulation should replace Epidyolex for approved epilepsy indications or that it will work better for psychiatric, sleep, pain, or inflammation targets.
Questions About CBD Powder vs. Epidyolex
Did CBtru CBD powder outperform Epidyolex?
It outperformed Epidyolex on absorption timing and several fasted metabolite-exposure measures. It did not clearly outperform Epidyolex on fed-state parent-CBD exposure, and it did not test clinical outcomes.
Does faster CBD absorption mean stronger treatment?
Not by itself. Faster absorption can change onset timing and peak-related tolerability, but clinical benefit depends on indication, dose, repeated dosing, exposure-response relationships, and adverse-effect tradeoffs.
Should CBD be taken with food?
For oral purified CBD, food state has a large effect on exposure. The 2026 trial found about 3.0-fold to 3.5-fold higher CBD exposure after a high-fat meal than after fasted dosing, matching prior CBD pharmacokinetic work. Patients using prescription CBD should follow the product-specific dosing instructions from their prescriber because consistency matters.
Does this apply to over-the-counter CBD products?
Only partly. The trial tested 2 standardized 400-mg pharmaceutical-style formulations under supervised conditions. Commercial CBD products vary by dose accuracy, excipients, route, contamination risk, cannabinoid content, and labeling quality, so the numbers cannot be transferred directly to retail products.
References
- Bendik I, Beck M, Manderna A, et al. Comparative pharmacokinetics and safety of cannabidiol in a powder formulation, CBtru, vs. an oil-based formulation, Epidyolex, under fasted and fed conditions in healthy participants: a randomized open-label cross-over Phase I study. CNS Drugs. 2026;40:709-723. doi:10.1007/s40263-026-01280-1
- Taylor L, Gidal B, Blakey G, Tayo B, Morrison G. A Phase I, randomized, double-blind, placebo-controlled, single ascending dose, multiple dose, and food effect trial of the safety, tolerability and pharmacokinetics of highly purified cannabidiol in healthy subjects. CNS Drugs. 2018;32(11):1053-1067. doi:10.1007/s40263-018-0578-5
- Crockett J, Critchley D, Tayo B, Berwaerts J, Morrison G. A phase 1, randomized, pharmacokinetic trial of the effect of different meal compositions, whole milk, and alcohol on cannabidiol exposure and safety in healthy subjects. Epilepsia. 2020;61(2):267-277. PubMed
- Saals B, De Bie TH, Osmanoglou E, et al. A high-fat meal significantly impacts the bioavailability and biphasic absorption of cannabidiol (CBD) from a CBD-rich extract in men and women. Scientific Reports. 2025;15:3678. PubMed
- Izgelov D, Davidson E, Barasch D, Regev A, Domb AJ, Hoffman A. Pharmacokinetic investigation of synthetic cannabidiol oral formulations in healthy volunteers. European Journal of Pharmaceutics and Biopharmaceutics. 2020;154:108-115. PubMed
- Schultz HB, Hosseini A, McLachlan AJ, Reuter SE. Population pharmacokinetics of oral-based administration of cannabidiol in healthy adults: implications for drug development. Cannabis and Cannabinoid Research. 2023;8(5):877-886. PubMed
Leave a Reply