A 2026 emergency department claims analysis estimated 3.87 million United States ED visits in 2021 where take-home naloxone could have been clinically relevant, compared with 226,453 ED-treated opioid-overdose visits in the same database.1 The finding reframes naloxone distribution as an emergency-care workflow for overdose risk, polysubstance exposure, long-term opioid use, and patients who arrive after an opioid overdose.
Research Highlights
- At-risk visits were much broader than overdose visits: the analysis estimated 3.87 million ED visits eligible for naloxone consideration, while 226,453 visits involved opioid overdose treated in the ED.
- Most opportunity was outside the overdose code: about 3.64 million at-risk visits were not classified as opioid-overdose encounters.
- Nonopioid drug use was a major route into risk: nonopioid drug use accounted for more than 23% of all estimated naloxone-relevant ED visits, reflecting fentanyl contamination and polysubstance risk.
- Public coverage carried most visits: Medicare or Medicaid paid for 65.2% of the estimated at-risk ED visits, which makes pharmacy access and discharge-kit policy central implementation issues.
- Evidence strength is operational: 2021 claims data can estimate visit-level opportunity for naloxone programs, but claims cannot prove that a specific kit prevented overdose after discharge.
Naloxone is an opioid-reversal medication that can restore breathing during an overdose by displacing opioids from receptors in the brain and body. It does not treat opioid use disorder, withdrawal, or stimulant toxicity. Its value is narrower and more urgent: when respiratory depression is opioid-mediated, having naloxone nearby can turn a fatal event into a survivable emergency.
Mannerings et al. used the 2021 Healthcare Cost and Utilization Project Nationwide Emergency Department Sample, a United States all-payer ED database, to estimate how many ED visits would meet expert-derived criteria for naloxone distribution.1 The study included 30,099,368 visit records from 993 hospitals in 41 states, then used national weighting to estimate United States ED burden.
3.87 Million ED Visits Met Naloxone-Relevant Risk Criteria
Researchers identified 3,869,699 ED visits, 95% confidence interval (CI) 3.62 million to 4.10 million, that matched at least 1 naloxone-relevant risk category. A confidence interval gives the range of estimates compatible with the sample and statistical design; here, even the lower bound remained far larger than opioid-overdose encounters alone.
The opioid-overdose comparison was the anchor. In the same database, 226,453 ED visits involved opioid overdose treated in the ED. The Centers for Disease Control and Prevention estimate for nonfatal opioid-overdose ED visits was similar at 217,446, which gave the claims approach some external calibration.2
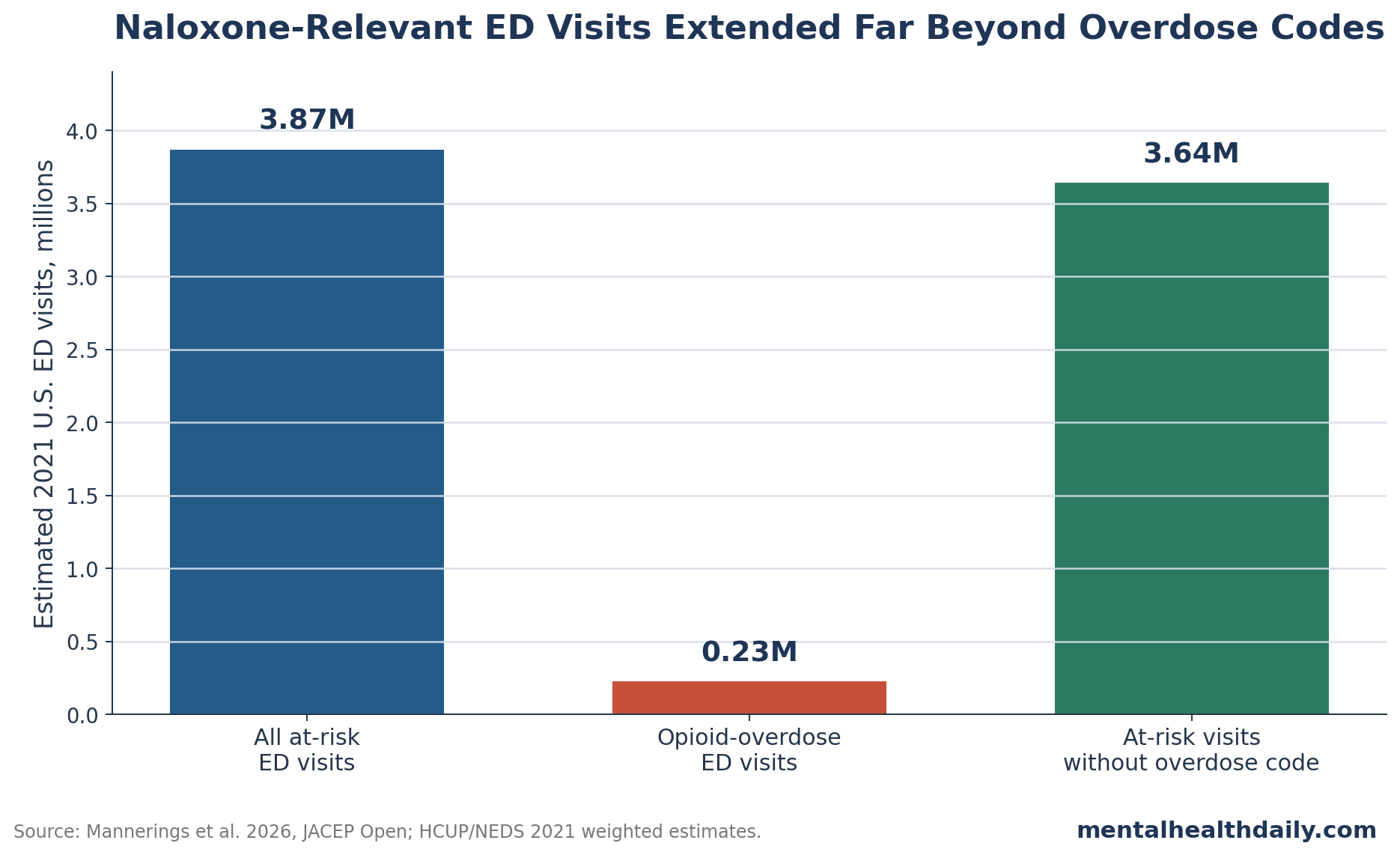
- All at-risk visits: 3.87 million ED encounters met criteria where naloxone distribution could be considered.
- ED-treated opioid overdose: 226,453 encounters were coded as opioid overdose in the Nationwide Emergency Department Sample.
- At-risk but not overdose-coded: roughly 3.64 million encounters met risk criteria without being classified as the overdose event itself.
The main clinical implication is that an overdose-only discharge policy captures a small slice of naloxone opportunity. A patient with cocaine use, benzodiazepine exposure, long-term opioid therapy, or opioid use disorder may leave the ED without an overdose diagnosis and still face opioid-related death risk after discharge.
Polysubstance Risk Makes Nonopioid Visits Relevant
Nonopioid drug-use encounters accounted for more than 23% of all estimated at-risk visits. The United States overdose market no longer separates cleanly into opioid and nonopioid lanes: fentanyl has appeared in stimulant supplies, and people using methamphetamine, cocaine, benzodiazepines, or multiple substances may be exposed to opioids intentionally or unintentionally.3
Mechanism: naloxone only reverses the opioid component of toxicity. If an ED visit involves stimulant intoxication plus fentanyl exposure, naloxone can treat respiratory depression from fentanyl while leaving stimulant agitation, hyperthermia, or arrhythmia risk untouched. That partial protection is still clinically valuable because the respiratory component is often the immediate lethal pathway.
The visit-type split also showed why a narrow opioid label can undercount risk:
- Nonopioid category: 46.3% of estimated at-risk visits, or 1,790,861 visits.
- Opioid category: 46.2% of estimated at-risk visits, or 1,788,947 visits.
- Both opioid and nonopioid categories: 7.5% of estimated at-risk visits, or 289,890 visits.
The shared opioid-plus-nonopioid group is small relative to the 2 larger categories, but it points to a practical problem in ED triage: a patient may appear under a stimulant, sedative, psychiatric, pain, or injury label while still being the right person to receive naloxone education and a take-home kit.
Medicaid and Medicare Paid for Nearly 2 in 3 At-Risk Visits
Payer mix: The payer data connect clinical screening to implementation. Medicaid paid for 40.2% of estimated at-risk visits, or 1,554,842 visits. Medicare paid for 25.0%, or 969,067 visits. Together, Medicare and Medicaid covered 65.2% of the estimated naloxone-relevant ED volume.
Program design: That concentration matters for program design. If a hospital relies on patients filling prescriptions later, the ED has handed the most fragile part of the workflow to pharmacy access, transportation, insurance formulary rules, copays, stigma at the counter, and patient follow-through after an acute visit. Direct ED dispensing or discharge kits can bypass several of those steps.
Prior work has found that ED naloxone programs can be implemented, but real-world uptake depends on staff workflow, kit availability, counseling scripts, and whether clinicians see overdose prevention as part of emergency care.45 The 2026 estimate adds scale: if the denominator is millions of visits, small workflow frictions become large missed prevention volume.
Adults 35 to 54 Made Up 38.2% of At-Risk Visits
Age pattern: The age distribution was concentrated in adults who often intersect with pain care, substance-use treatment, and chronic disease management. People aged 35 to 54 accounted for 38.2% of at-risk visits. People aged 19 to 34 accounted for 27.3%. Adults aged 55 to 64 contributed 17.5%, and adults aged 65 or older contributed 15.3%.
Race-data caveat: People of color accounted for 39.3% of estimated at-risk visits, though race and ethnicity data were incomplete in the claims source. Researchers warned that racial coding gaps can distort subgroup estimates. That limitation does not remove the implementation point: ED naloxone programs need consistent delivery rules so access does not depend on whether a clinician personally labels a patient as a likely overdose risk.
Evidence strength: this was a retrospective claims analysis, so it estimates where naloxone distribution could be considered. It cannot determine which patients actually received naloxone, which patients used it later, or how many deaths would be prevented by distributing kits to every eligible visit.
The code list also came from an expert panel rather than a full RAND/UCLA or Delphi consensus process. Claims codes can miss patient-level detail, duplicate repeat visits by the same person, and misclassify substance exposures. The result is still useful for planning because overdose-coded visits were externally close to the CDC estimate, while the broader risk categories exposed a much larger preventable-risk workflow.
Workflow design: a practical naloxone workflow needs 2 parts: a screening trigger and a distribution step. The screening trigger can be diagnosis-code based, clinician-entered, or embedded in the discharge process. The distribution step can be a prescription, an on-site kit, a bedside handoff from pharmacy, or a linkage to a community harm-reduction program.
Screening trigger: overdose diagnosis should be automatic, but the 2026 analysis argues for additional triggers such as opioid use disorder, long-term opioid therapy, nonopioid drug use with fentanyl exposure risk, and polysubstance use. A rule that waits for an overdose code leaves millions of risk-relevant visits untouched.
Distribution step: a prescription is weaker than a kit when the patient may not reach a pharmacy, may face cost barriers, or may avoid a stigmatizing interaction. ED-based kit distribution creates inventory, training, and documentation work, but it also closes the gap between identifying risk and placing naloxone in hand.
Education has to be short enough for discharge reality. The minimum viable counseling package is how to recognize slow or stopped breathing, how to administer naloxone, why repeat dosing may be needed with fentanyl, why emergency services should still be called, and why rescue breathing or airway positioning can matter while waiting for help.
Questions About ED Naloxone Distribution
Does naloxone help with stimulant overdose?
Naloxone reverses opioid-driven respiratory depression. It does not reverse stimulant toxicity itself, but it can still help when fentanyl or another opioid is mixed into stimulant use.
Why would an ED give naloxone after a non-overdose visit?
The goal is prevention after discharge. Long-term opioid use, opioid use disorder, prior overdose, polysubstance exposure, and some nonopioid drug-use encounters can identify people who may face opioid overdose later.
Did this study prove that ED naloxone kits prevent deaths?
No. The study estimated naloxone-relevant ED visit volume from claims data. Mortality prevention would need separate outcome studies that follow patients after discharge.
What is the strongest operational takeaway?
Overdose-only policies are too narrow for ED naloxone distribution. Screening rules need to include opioid use disorder, long-term opioid use, polysubstance risk, and nonopioid drug-use encounters where fentanyl exposure is plausible.
References
- Estimating the Need for Naloxone Distribution from United States Emergency Departments. Mannerings AM et al. JACEP Open. 2026;7(2):100365. doi:10.1016/j.acepjo.2026.100365
- Emergency Department Visit Rates for Nonfatal Opioid Overdose. Cairns C et al. NCHS Data Brief. 2023. PubMed:37642973
- Fentanyl, Heroin, and Cocaine Overdose Fatalities Involving Multiple Substances. Armenian P et al. MMWR. 2019;68(31):666-670. doi:10.15585/mmwr.mm6831a2
- A Novel Program for Dispensing Take-Home Naloxone in Emergency Departments. O’Brien DC et al. BMC Health Services Research. 2019;19:682. doi:10.1186/s12913-019-4469-3
- National Prevalence of Naloxone Prescribing in U.S. Emergency Departments and Affiliated Pharmacies. Suen LW et al. Journal of General Internal Medicine. 2022;37:1220-1228. doi:10.1007/s11606-021-07069-w
- A Qualitative Study on Naloxone Access in Emergency Departments. Bazazi AR et al. Journal of Urban Health. 2024;101:699-713. doi:10.1007/s11524-024-00852-0
Leave a Reply