A 2026 target-trial emulation involving 102,361 U.S. veterans with type 2 diabetes found no increased suicidality risk after starting semaglutide vs. sodium-glucose cotransporter-2 inhibitors (SGLT2 inhibitors): suicidal ideation HR 0.99 and suicide attempt/death HR 1.05 after overlap weighting.1 That does not prove semaglutide prevents suicide, but it weakens the broad claim that semaglutide initiation itself raises suicide risk in this high-risk diabetes cohort.
Research Highlights
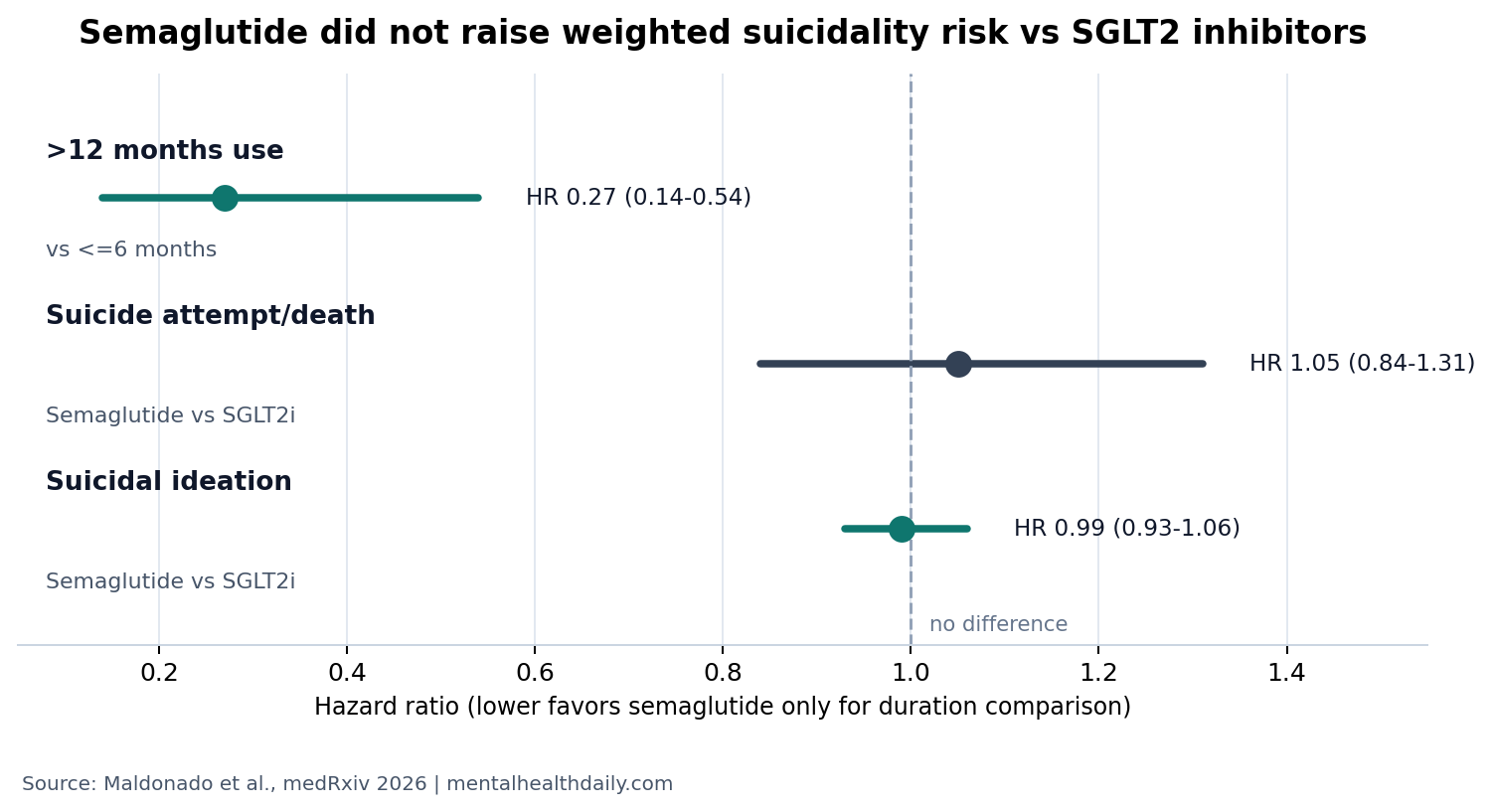
- No weighted ideation increase: semaglutide initiation had suicidal ideation HR 0.99 (95% CI 0.93-1.06; P = 0.86) vs. SGLT2 inhibitor initiation in 102,361 veterans.1
- Severe events stayed statistically similar: suicide attempt/death HR was 1.05 (95% CI 0.84-1.31) after weighting, even though crude event rates were higher before confounding adjustment.1
- Baseline selection explained much of the crude signal: semaglutide initiators had 56.3 ideation events per 1,000 person-years vs. 36.8 for SGLT2 inhibitor initiators before weighting.1
- Sustained use looked lower-risk, not higher-risk: more than 12 months of continuous semaglutide use had suicide attempt/death HR 0.27 vs. 6 or fewer months, but adherence analyses can carry healthy-user bias.1
- Class-wide alarm lacked support: 2024-2025 real-world and meta-analytic studies also failed to show a consistent GLP-1 suicidality increase.2,3,4
Semaglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist, meaning it activates an incretin hormone pathway that increases glucose-dependent insulin secretion, slows gastric emptying, reduces appetite, and can produce major weight loss. The suicide-risk question became clinically noisy because GLP-1 drugs moved from diabetes treatment into mass weight-loss use, while product warnings and pharmacovigilance reports raised concerns about suicidal thoughts or behavior.
Target-trial emulation uses observational data to imitate the design logic of a randomized trial: define eligibility, treatment start, comparator, follow-up, outcomes, and adjustment before estimating treatment effects. It is stronger than a loose database association, but it still cannot balance factors the database did not measure.
102,361 Veterans Showed No Weighted Semaglutide Suicidality Increase
Maldonado et al. used Veterans Health Administration records from March 1, 2018 to March 1, 2025 to compare 11,478 new semaglutide initiators with 90,883 new SGLT2 inhibitor initiators.1 The comparator matters: SGLT2 inhibitors are diabetes drugs with cardiovascular and kidney benefits, so the contrast was not semaglutide vs. no treatment.
Overlap weighting is a statistical balancing method that gives more influence to patients whose measured characteristics make either treatment plausible. Before that weighting, semaglutide users looked riskier: suicidal ideation occurred at 56.3 per 1,000 person-years among semaglutide initiators vs. 36.8 among SGLT2 inhibitor initiators, and suicide attempt/death occurred at 4.30 vs. 2.64 per 1,000 person-years.
After weighting, the difference essentially disappeared. Suicidal ideation had HR 0.99, 95% CI 0.93-1.06, P = 0.86. Suicide attempt/death had HR 1.05, 95% CI 0.84-1.31. The composite suicidality result was also not elevated after adjustment.
Event counts make the severe-outcome estimate readable: the analysis captured 9,077 suicidal ideation events and 696 suicide attempt/death events during a median 2.2 years of follow-up.1 That is enough information to make a large hidden hazard less likely, but the wider confidence interval for attempt/death still leaves room for smaller effects that this observational design cannot pin down.
The crude pattern and the weighted pattern are the core lesson. Semaglutide patients had more observed psychiatric risk before adjustment, but the adjusted comparison did not support semaglutide initiation as the reason for that higher crude event rate.
Why SGLT2 inhibitors are a useful comparator: they are not inert pills, and they are not psychiatric drugs. They are glucose-lowering medications with cardiorenal benefits, prescribed to many of the same type 2 diabetes patients who might also be considered for semaglutide.
Comparing semaglutide with SGLT2 inhibitors therefore reduces one common bias in diabetes pharmacoepidemiology: the tendency to compare a newer, more intensively managed drug group with patients receiving no similar second-line treatment.
Sustained Semaglutide Use Looked Safer Than Short Use, but Selection Is Hard to Remove
The researchers also used clone-censor-weight methods to compare duration of continuous semaglutide use among semaglutide initiators: 6 or fewer months, 7-12 months, and more than 12 months.1 Compared with 6 or fewer months, more than 12 months of continuous semaglutide use was associated with lower suicide attempt/death risk, HR 0.27, 95% CI 0.14-0.54, P < .001. The 7-12 month arm had HR 0.56, 95% CI 0.25-1.23, P = .15.
That duration analysis is reassuring against a simple cumulative-toxicity story: if semaglutide were steadily raising severe suicidality risk, longer continuous use should not obviously look safer than early discontinuation. The finding also fits a possibility that metabolic improvement, weight loss, lower inflammation, or closer care engagement could reduce severe distress for some patients.
Interpretive limit: people who remain on a medication for more than 12 months can differ from people who stop early. They may tolerate the drug better, have fewer adverse effects, stay more connected to care, or be healthier in ways the model cannot fully measure. The duration result is a signal against obvious accumulating harm, not proof that semaglutide itself prevents suicide attempt or death.
Discontinuation is hard to interpret: some patients stop because of nausea, access problems, cost, weight-loss disappointment, or medication shortages. Others may stop because psychiatric symptoms, medical instability, or life stress disrupt adherence.
A database can model measured covariates, but it cannot fully tell whether discontinuation caused worse outcomes or whether worsening health made discontinuation more likely.
Real-World and Meta-Analytic GLP-1 Evidence Mostly Points the Same Way
Wang et al. used a large real-world cohort and reported lower suicidal ideation risk among semaglutide users compared with non-GLP-1 medications in obesity and type 2 diabetes cohorts.2 That study asked a similar safety question but used different comparators and a different data source.
Ebrahimi et al. reviewed suicide and self-harm events with GLP-1 receptor agonists in adults with diabetes or obesity and did not find a clear increased-risk signal, while emphasizing sparse event counts and the limits of safety reporting.3 Valentino et al. similarly reviewed GLP-1 receptor agonists and suicidality measures and did not identify consistent worsening across available studies.4
Taken together, the adjacent evidence makes a class-wide suicidality warning look less empirically convincing than the public anxiety around it. The better safety stance is narrower: monitor mood and suicidal thoughts in patients at risk, but do not treat semaglutide initiation as proven to increase suicidality based on the current evidence.
Patient-specific risk still matters: a null average safety signal still leaves room for patient-specific distress during treatment. Rapid appetite change, gastrointestinal distress, body-weight change, diabetes complications, pain, alcohol use, depression, social isolation, and medication access can all shape a person’s suicide risk outside the drug mechanism itself.
The evidence argues against a broad drug-level alarm, while leaving ordinary clinical vigilance intact.
That is the practical middle ground. The available evidence does not support stopping semaglutide solely because of a generalized suicidality rumor, and it also does not support ignoring new mood symptoms after any medication change. The correct response is targeted monitoring for people with recent suicidal thoughts, major depression, substance-use instability, severe nausea, rapid weight change, or disrupted access to diabetes care.
Veterans With Diabetes Are Not the Same as Every Weight-Loss Patient
This study is valuable partly because veterans have elevated baseline suicide risk and the cohort included 696 suicide attempt/death events during a median 2.2 years of follow-up.1 A safety signal that fails to appear in a high-risk system deserves attention.
The scope is still specific. The analysis covered U.S. veterans with type 2 diabetes initiating semaglutide in VHA care. It does not automatically answer whether semaglutide affects mood in younger patients, non-veterans, people using GLP-1 drugs only for weight loss, or patients with recent medication changes, eating disorders, severe nausea, rapid weight change, or active suicidal crisis.
Evidence-strength note: the paper was a preprint at extraction time and was not randomized. The strongest conclusion is that measured real-world VHA data do not show higher suicidality after semaglutide initiation vs. SGLT2 inhibitor initiation. The study cannot replace patient-level suicide-risk assessment.
Questions About Semaglutide and Suicide Risk
Did semaglutide increase suicidal ideation in this veteran diabetes study?
No. After overlap weighting, suicidal ideation was essentially identical for semaglutide vs. SGLT2 inhibitor initiators: HR 0.99, 95% CI 0.93-1.06.
Did semaglutide increase suicide attempts or deaths?
The weighted severe-event estimate was not statistically elevated: HR 1.05, 95% CI 0.84-1.31. Severe events were rare, so individual clinical monitoring still matters.
Does longer semaglutide use protect against suicide?
Not proven. More than 12 months of continuous use was associated with lower suicide attempt/death risk, HR 0.27 vs. 6 or fewer months, but adherence analyses can reflect who stays on treatment rather than only what the drug does.
What should clinicians and patients do with this evidence?
The data support routine mood and suicide-risk monitoring without treating semaglutide as a confirmed suicidality trigger. Patients with new or worsening suicidal thoughts need urgent clinical assessment regardless of which diabetes or weight-loss medication they are taking.
References
- Maldonado AI, et al. Semaglutide Initiation and Treatment Duration Are Not Associated with Increased Suicidality Risk in Veterans with Type 2 Diabetes. medRxiv. 2026. doi:10.64898/2026.04.17.26351118
- Wang W, Volkow ND, Berger NA, Davis PB, Kaelber DC, Xu R. Association of semaglutide with risk of suicidal ideation in a real-world cohort. Nature Medicine. 2024;30(1):168-176. doi:10.1038/s41591-023-02672-2
- Ebrahimi P, Batlle JC, Ayati A, et al. Suicide and self-harm events with GLP-1 receptor agonists in adults with diabetes or obesity: a systematic review and meta-analysis. JAMA Psychiatry. 2025;82(9):888-895. doi:10.1001/jamapsychiatry.2025.0091
- Valentino K, Teopiz KM, Cheung W, et al. The effect of glucagon-like peptide-1 receptor agonists on measures of suicidality: a systematic review. Journal of Psychiatric Research. 2025;183:112-126. doi:10.1016/j.jpsychires.2025.02.008
Leave a Reply