
⏱ 8 min read
A 228-person randomized trial found a split result for workplace mental-health apps: executive-function training reduced anxiety and depressive symptoms at 12-week follow-up, while a self-guided CBT app improved workplace wellbeing without reducing symptoms.1 The mechanism claim was weaker than the outcome claim because measured executive-function change did not explain the improvements.
Research Highlights
- 228 adults were randomized: MacLellan et al. recruited working adults with mild-to-moderate depression and anxiety symptoms, including 147 women.1
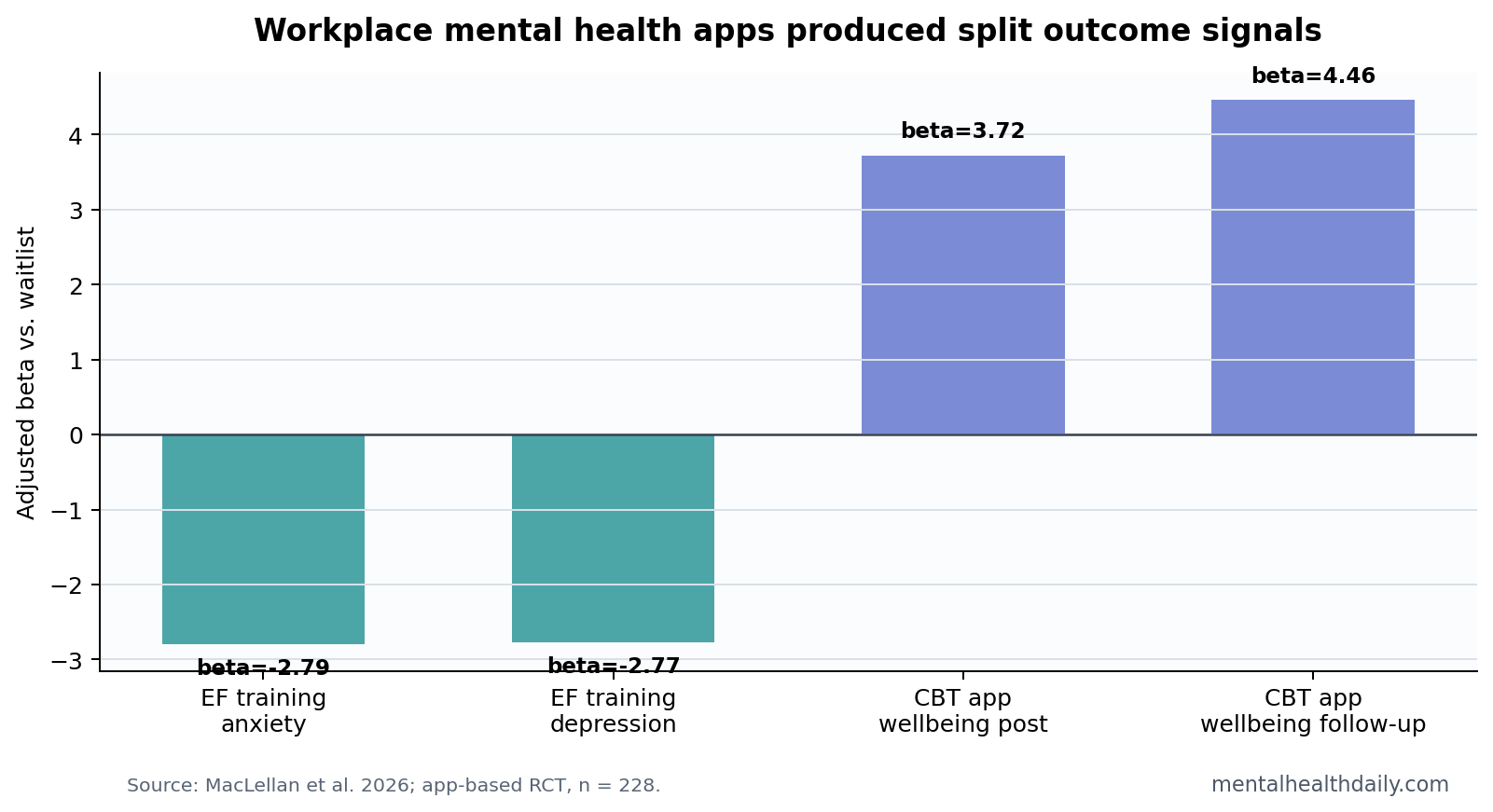
- Executive-function training reduced symptoms later: anxiety improved at follow-up, beta = −2.79, p = 0.004, and depressive symptoms improved, beta = −2.77, p = 0.02.1
- CBT app effects were work-focused: self-guided CBT improved workplace wellbeing at postintervention, beta = 3.72, p = 0.02, and follow-up, beta = 4.46, p = 0.02.1
- Mediation was not supported: executive-function change did not explain symptom or wellbeing changes, which weakens the proposed brain-training pathway.1
- Attrition limits certainty: 58% missingness at follow-up means durability needs replication in a less leaky trial.1
Executive-function training means repeated computerized tasks intended to improve cognitive control, working memory, and related skills. In depression and anxiety, the theory is that better cognitive control might reduce rumination, worry, and difficulty shifting attention away from threat or negative information.
Self-guided CBT apps translate cognitive behavioral therapy exercises into unguided phone modules. They can help users track thoughts, behavior, mood, and coping plans, but they remove the therapist relationship and real-time clinical adjustment that ordinary CBT provides.
Executive-Function Training Helped Symptoms at 12 Weeks
The executive-function app did not show immediate postintervention symptom reductions, but follow-up scores moved. Anxiety improved by beta = −2.79, p = 0.004, and depressive symptoms improved by beta = −2.77, p = 0.02, relative to waitlist control.1
That delayed pattern is plausible if repeated practice changes coping or attentional habits slowly. It is also compatible with nonspecific app engagement, regression to the mean, or selective retention. Follow-up missingness was high enough that the durability claim needs caution.
The CBT App Improved Workplace Wellbeing, Not Symptoms
The self-guided CBT app did not significantly reduce depression or anxiety symptoms. Its clearer signal was workplace wellbeing: beta = 3.72 at postintervention and beta = 4.46 at follow-up, both p = 0.02.1
That pattern should not be treated as failure. Workplace wellbeing is not a soft endpoint when the intervention is sold for work functioning. It may capture social connection, meaning, engagement, and perceived work capacity that symptom scales miss.
Digital-intervention reviews have already shown that symptom effects vary across programs, support levels, populations, and engagement patterns.2 This trial adds a useful split: symptom reduction and work wellbeing may not move in the same app arm.
Executive Function Did Not Explain the Improvement
The most important negative result is the mediation failure. Mediation asks whether the intervention changed an intermediate process that then explained the clinical outcome. Here, executive-function improvement did not mediate changes in symptoms or workplace wellbeing.1
That finding keeps the article from becoming a brain-training success story. Meta-analytic work on working-memory training has long warned that transfer to broad life outcomes is difficult to prove.4 A symptom benefit without mediation may still be real, but the mechanism probably needs a different explanation.
Digital Workplace Programs Need Outcome-Specific Claims
Evidence-strength note: this was a randomized trial, which is stronger than a user-satisfaction study. Attrition, self-guided delivery, and high follow-up missingness still limit confidence.
Employers and clinicians should avoid treating all mental-health apps as interchangeable. A program can reduce symptoms, improve workplace functioning, improve neither, or improve one while missing the other.
- For symptom care: depression and anxiety scales need to move alongside engagement metrics.
- For workplace wellbeing: work-specific outcomes should be measured directly.
- For mechanism claims: mediation analyses should support the proposed pathway before marketing repeats it.
Why the Negative Mediation Result Is Useful
A negative mediation result can be more informative than another small app effect. If executive-function training reduced symptoms but measured executive-function change did not explain the reduction, the intervention may be working through another pathway or through nonspecific engagement.
Possibilities include expectancy, daily routine, brief distraction from worry, a sense of progress, or repeated contact with a structured task. None of those explanations would make the symptom result fake. They would simply mean the app should not be marketed as improving depression through proven executive-function repair.
That distinction is important for workplace programs because mechanism claims often drive purchasing. A company may buy “cognitive control” training because it sounds more biological and scalable than ordinary self-help. The trial says the biological-sounding pathway was not demonstrated.
Workplace Wellbeing Is Not the Same Endpoint as Mental Health Symptoms
Workplace wellbeing can improve without large PHQ-9 or GAD-7 changes. A person might feel more connected to coworkers, more capable of handling tasks, or more aligned with work goals while still endorsing low mood or worry. Conversely, symptoms can improve while work engagement remains impaired by workload, management, scheduling, or job insecurity.
That is why the CBT app result deserves a separate interpretation. It may have helped users organize work stress, reframe work problems, or act with more intention in the workplace without producing enough symptom change to move depression or anxiety scales.
Endpoint matching: app trials should state the endpoint they are built to change. If a program promises depression treatment, PHQ-9 or an equivalent symptom scale should be central. If it promises workplace wellbeing, work-specific wellbeing, absenteeism, presenteeism, and perceived work functioning should be central.
Attrition Is Part of the Intervention, Not a Footnote
Digital mental-health studies often separate efficacy from engagement, but users experience them together. A self-guided program that works only for the minority who complete it may still be valuable, but its population-level effect depends on who drops out and why.
The 58% follow-up missingness in this trial weakens confidence in late symptom effects.1 Missing data can exaggerate benefit if people who improve are more likely to respond. It can also hide benefit if people who struggle remain in the data while people who quietly recover disengage. The problem is not that attrition proves bias in one direction; the problem is that it widens the uncertainty around the estimate.
For employers, the audit question is concrete: how many workers start, how many complete, who benefits, who drops out, and whether the program routes high-risk users toward human support.
Self-Guided Apps Should Not Carry Clinical Work Alone
Self-guided workplace apps are attractive because they scale cheaply and avoid scheduling barriers. They are also easy to overdeploy. A phone app cannot fix an abusive manager, impossible workload, insecure employment, or untreated severe depression.
The trial’s split outcome should sharpen implementation. If an employer offers a CBT app for workplace wellbeing, the surrounding system should still include confidential clinical referral, workload review, crisis pathways, and protection against using app participation as a productivity surveillance tool.
Privacy boundary: workplace mental-health programs should report aggregate uptake and outcomes, not individual distress scores to managers. Without that boundary, employees may avoid precisely the tools they need because the tool becomes another source of monitoring.
Clinical boundary: mild-to-moderate symptoms are not the same as suicidal risk, psychosis, mania, substance withdrawal, or severe functional collapse. A workplace app can be one low-friction access point, but it should route high-risk users toward human care rather than asking a self-guided module to carry clinical triage.
That routing should be explicit before rollout. Employees should know what happens when risk is disclosed, who can see the data, and which support path exists outside the app.
Implementation endpoint: a workplace app should be judged partly by what it triggers outside the phone. If symptom scores worsen, does the program recommend clinical care? If a worker reports overload, does the employer have any workload intervention? If the answer is no, the app becomes a narrow self-management tool sitting inside the same work conditions that may be sustaining distress.
Scope of benefit: self-guided tools can still teach coping skills, structure reflection, and lower access barriers for mild symptoms.
The claim should match the deployment setting. An app cannot substitute for staffing, management reform, confidential care pathways, or accommodations when the workplace itself is part of the problem.
Workers also need an opt-out path that does not mark them as uncooperative or less committed to the employer’s wellbeing program.
The research implication is equally direct. Future trials should separate app efficacy from workplace governance. A program can be psychologically coherent and still fail in a workplace where employees do not trust how their data will be used.
Questions About Workplace Mental Health Apps
Did the CBT app reduce depression or anxiety?
No clear symptom reduction was found for the self-guided CBT app in this trial, although workplace wellbeing improved.
Did executive-function training work because executive function improved?
The trial did not support that mechanism. Symptoms improved at follow-up, but measured executive-function change did not explain the effect.
Should employers buy apps based only on engagement?
No. High adherence is encouraging, but app claims should be tied to the outcome being promised: symptoms, work wellbeing, absenteeism, presenteeism, or another explicit endpoint.
References
- MacLellan A, Fairchild G, Button KS. The effectiveness and mechanisms of action of app-based interventions for improving mental health and workplace well-being: randomized controlled trial. JMIR Mental Health. 2026;13:e91564. https://doi.org/10.2196/91564
- Moshe I, et al. Digital interventions for the treatment of depression: a meta-analytic review. Psychological Bulletin. 2021;147:749-786. https://doi.org/10.1037/bul0000334
- Domhardt M, et al. Therapeutic processes in digital interventions for anxiety: a systematic review and meta-analytic structural equation modeling. Clinical Psychology Review. 2021;90:102084. https://doi.org/10.1016/j.cpr.2021.102084
- Melby-Lervag M, Redick TS, Hulme C. Working memory training does not improve performance on measures of intelligence or other measures of far transfer. Perspectives on Psychological Science. 2016;11:512-534. https://doi.org/10.1177/1745691616635612
Leave a Reply