⏱ 8 min read
A 2026 medRxiv case-control study found that serum myelin oligodendrocyte glycoprotein was 20.5 pg/ml higher in multiple sclerosis than in healthy donors and 15.3 pg/ml higher during relapse than remission, making it a plausible blood marker of demyelination rather than a replacement for neurofilament light chain.
Research Highlights
- MOG was higher in MS: serum myelin oligodendrocyte glycoprotein was 20.5 pg/ml higher in treatment-naive relapsing MS than in matched healthy donors, with an ROC AUC of 0.85.
- Relapse signal was visible: relapse samples had 15.3 pg/ml higher serum MOG than remission samples, while NfL was also higher during relapse.
- MOG added to NfL: high NfL alone identified 48.6% of relapse samples, but high MOG or high NfL identified 57%; 8.6% were high-MOG-only.
- OND controls calibrated specificity: MOG separated MS from other neurological disease controls with an AUC of 0.82, while NfL discrimination was weak at AUC 0.61.
- Evidence is still early: the 2026 preprint used archived samples, retrospective design, and incomplete matching, keeping serum MOG out of routine clinical decision-making for now.
Serum MOG means myelin oligodendrocyte glycoprotein protein measured in blood. MOG sits on the outer surface of central nervous system myelin, the insulating sheath around nerve fibers, so a rise in circulating MOG protein could mark myelin damage more directly than a general nerve-injury marker.
That is different from MOG-IgG antibody testing, which looks for immune antibodies used to diagnose MOG antibody-associated disease. Oh et al. were not testing whether MS patients had MOGAD. They were asking whether MOG protein itself behaves like a blood biomarker for MS diagnosis and relapse activity.
Serum MOG Was Higher in Multiple Sclerosis Than in 2 Control Groups
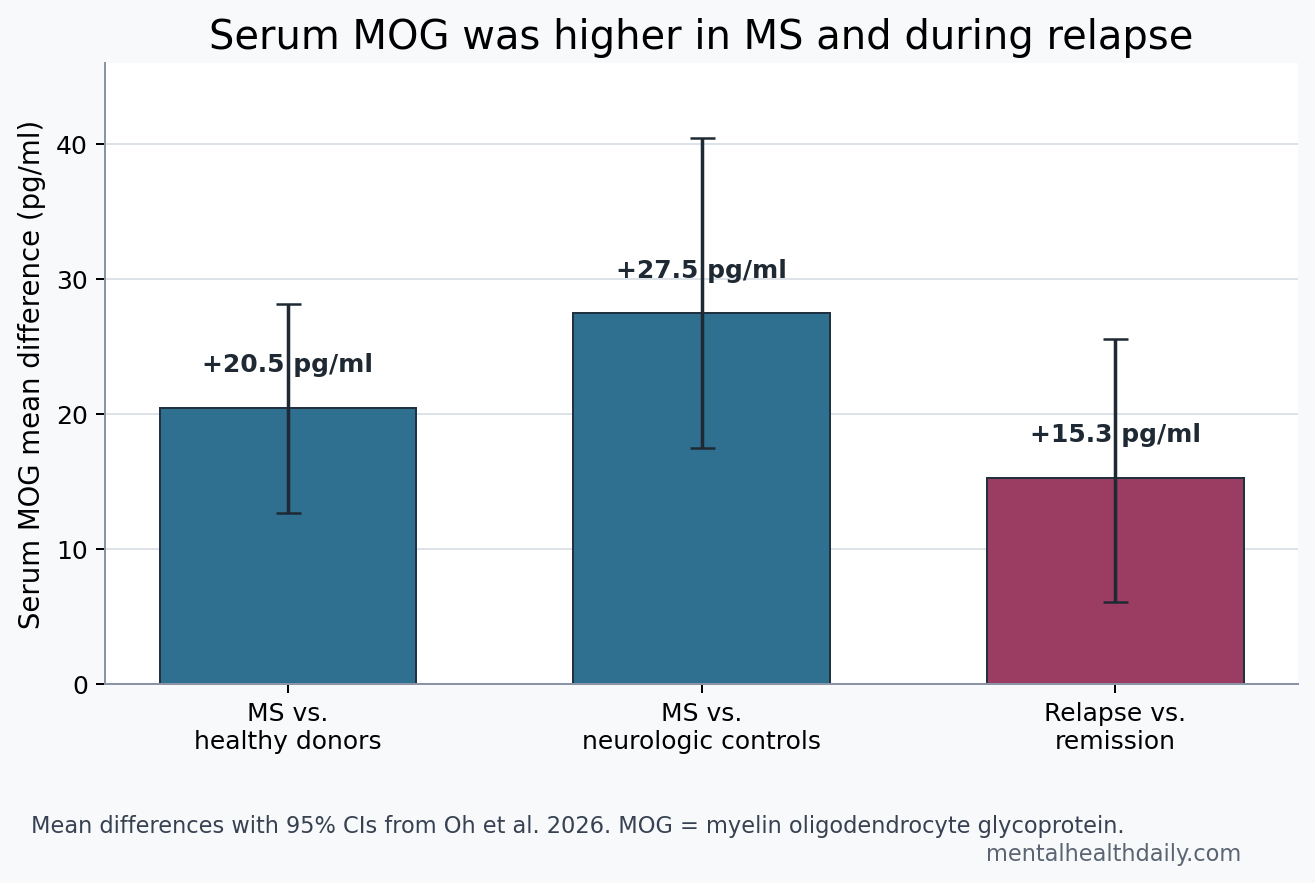
Oh et al. tested archived serum from 2 biorepositories. The first comparison used 33 treatment-naive people with relapsing-remitting multiple sclerosis and 35 age-, sex-, and race-matched healthy donors. Mean serum MOG was 62.0 pg/ml in MS vs. 41.5 pg/ml in healthy donors, a mean difference of 20.5 pg/ml (95% CI 12.7 to 28.2; p < 0.0001).
Receiver operating characteristic analysis asks how well a marker separates 2 groups across possible cutoffs. In the healthy-donor comparison, serum MOG produced an area under the curve (AUC) of 0.85 (95% CI 0.75 to 0.95). An AUC of 0.5 is no better than chance; 0.85 is a strong research signal, though not automatically a clinical test.
The second comparison was harder. Researchers compared 30 treatment-naive MS samples with 42 other neurological disease controls, including headache syndromes, dementia, motor neuron disease, neuropathy, and stroke. MOG was again higher in MS: 63.8 pg/ml vs. 35.9 pg/ml, a mean difference of 27.5 pg/ml (95% CI 17.5 to 40.5; p < 0.0001).
The other-neurological-disease group was not perfectly matched; it was older and clinically more heterogeneous. After adjustment for age, sex, race, and body mass index, MS diagnosis still predicted higher MOG levels, with an adjusted estimate of 24.8 pg/ml (95% CI 14.2 to 35.4; p < 0.0001). That adjusted result is the useful calibration: group imbalance does not explain the whole signal, but the design still cannot prove diagnostic readiness.
MOG Looked More MS-Specific Than NfL Against Other Neurological Diseases
Neurofilament light chain (NfL) is a structural protein released when axons are injured. In MS, blood NfL is one of the most studied biomarkers because it tracks inflammatory disease activity, future relapse risk, and tissue injury, but it is not specific to MS. Stroke, neurodegeneration, traumatic injury, neuropathy, and many other nervous-system disorders can raise NfL.
That limitation appeared directly in the Oh et al. data. Against healthy donors, NfL separated MS well, with AUC 0.87. Against other neurological disease controls, NfL dropped to AUC 0.61 (95% CI 0.48 to 0.74; p = 0.125), which is weak discrimination. Serum MOG held up better against other neurological disease controls, with AUC 0.82 (95% CI 0.72 to 0.92; p < 0.0001).
The read is not “MOG beats NfL” in general. NfL has a much larger validation base and is already tied to prognosis in studies such as Benkert et al.’s individualized MS disease-activity modeling. The narrower point is that MOG protein may be more myelin-weighted, while NfL is more axonal-injury-weighted. A person with MS and a comorbid neurological disorder may need both axes interpreted together.
Relapse Samples Had Higher MOG, but the Added Signal Was Modest
The disease-activity analysis compared 35 relapse samples with 27 remission samples from the VCU MS biorepository. Mean serum MOG was 57.6 pg/ml during relapse vs. 42.3 pg/ml during remission, a mean difference of 15.3 pg/ml (95% CI 6.11 to 25.6; p = 0.019). Serum NfL also rose during relapse: 15.5 pg/ml vs. 7.0 pg/ml (p = 0.017).
Cutoff analysis made the incremental value clearer. Using a cutoff of 2 standard deviations above the healthy-donor mean, high MOG appeared in 28.6% of relapse samples. High NfL appeared in 48.6%. When either high MOG or high NfL counted, 57% of relapse samples were flagged. The gain came from 8.6% of relapse samples with high MOG but not high NfL.
- NfL-only pattern: 28.6% of relapse samples were high for NfL but not MOG, fitting an axonal-injury-dominant signal.
- MOG-only pattern: 8.6% were high for MOG but not NfL, suggesting a smaller subgroup where myelin injury may be visible before or without a strong axonal marker rise.
- Combined-marker pattern: 57% exceeded at least 1 cutoff, which is better sensitivity than either marker alone but still leaves many clinical relapse samples unflagged.
That last number keeps the result grounded. A combined MOG/NfL rule did not identify every relapse. It improved relapse-sample capture by a modest amount in a retrospective analysis.
MOG and NfL May Separate Myelin Injury From Axonal Injury
Oh et al. found a moderate serum MOG-NfL correlation across MS samples (Pearson r = 0.523; p < 0.0001). Moderate correlation makes biological sense: active MS lesions can damage myelin and axons in the same inflammatory episode. It also leaves room for mismatch, where one marker rises more than the other.
The researchers framed the mismatch as a possible window into lesion timing. MOG sits on exposed myelin surfaces, while NfL is released when axons are injured. If myelin injury tends to occur earlier and axonal injury peaks later, blood MOG could rise before NfL in some lesions. Fox et al.’s 2024 work on serum NfL timing supports the broader sampling problem: NfL can lag radiologic lesion activity by weeks.
Adjacent biomarker work points in the same multi-marker direction. Meier et al. compared serum glial fibrillary acidic protein (GFAP), a marker of astrocyte stress and glial injury, with NfL in MS progression.
Chitnis et al. tested broader inflammatory and neurodegenerative serum protein panels and found that combining proteins improved sensitivity for clinical and radiographic activity. Abdelhak et al. later reported that myelin injury can precede axonal injury and symptomatic onset in MS, which fits the MOG-before-NfL hypothesis without proving it in this specific cohort.
Endophenotype means a measurable biological trait that can divide a diagnosis into more specific subgroups. High-MOG/low-NfL and low-MOG/high-NfL patterns might eventually identify demyelination-dominant vs. axonal-injury-dominant MS activity. In this dataset, though, those patterns could just reflect when the blood sample was drawn relative to lesion formation.
Preprint and Case-Control Design Keep This Out of Routine Relapse Triage
Evidence-strength note: this was an archived-sample, retrospective case-control study, and the paper was a medRxiv preprint that had not been certified by peer review. It can support a biomarker hypothesis. It cannot support standalone diagnosis, routine relapse confirmation, or treatment escalation based on serum MOG protein.
Several limits matter before translating the finding into clinic:
- Control matching: healthy donors were well matched, but the other-neurological-disease controls were older and clinically mixed.
- Assay calibration: age- and body-mass-adjusted z-scores were available for NfL from prior models, but not for MOG.
- Clinical synchronization: relapse status was clinical; the study did not synchronize MOG and NfL levels with new MRI lesion timing in a prospective protocol.
- Generalizability: samples came from biorepositories, not a real-time diagnostic pathway with prespecified cutoffs and external validation.
The best near-term use is research triage: pair serum MOG with NfL, GFAP, MRI activity, clinical relapse timing, and treatment exposure to ask whether myelin-dominant injury has a measurable blood signature. The clinical version would need prospective sampling before, during, and after MRI-confirmed inflammatory activity.
Questions About Serum MOG in Multiple Sclerosis
Is serum MOG the same as MOG antibody testing?
No. Serum MOG protein measures a myelin-associated protein in blood. MOG antibody testing measures immune antibodies against MOG and is used in the differential diagnosis of MOG antibody-associated disease. The biomarker signal here is circulating MOG protein, not anti-MOG autoimmunity.
Did serum MOG diagnose multiple sclerosis?
No. It separated MS groups from controls in retrospective research samples, including AUC 0.85 vs. healthy donors and AUC 0.82 vs. other neurological disease controls. That is not the same as a validated diagnostic test for individual patients.
Why pair MOG with NfL?
MOG may reflect myelin injury, while NfL reflects axonal injury. Pairing them could help distinguish lesion biology or sampling timing, especially when NfL is normal despite active demyelination or when NfL is elevated by another neurological condition.
What result would make serum MOG clinically stronger?
A prospective study would need to show that serum MOG rises before or during MRI-confirmed MS activity, adds prediction beyond NfL and GFAP, works across independent cohorts, and improves a real decision such as relapse triage or treatment monitoring.
References
- Oh U, Kwegyir-Aggrey A, Mufti F, Dintino C, Buxhoeveden S, McVoy J, et al. Serum myelin oligodendrocyte glycoprotein as an indicator of diagnosis and disease activity in multiple sclerosis. medRxiv. 2026. doi:10.1101/2025.09.06.25335236
- Benkert P, Meier S, Schaedelin S, et al. Serum neurofilament light chain for individual prognostication of disease activity in people with multiple sclerosis: a retrospective modelling and validation study. Lancet Neurology. 2022;21:246-257. PubMed
- Meier S, Willemse EAJ, Schaedelin S, et al. Serum glial fibrillary acidic protein compared with neurofilament light chain as a biomarker for disease progression in multiple sclerosis. JAMA Neurology. 2023;80:287-297. PubMed
- Chitnis T, Qureshi F, Gehman VM, et al. Inflammatory and neurodegenerative serum protein biomarkers increase sensitivity to detect clinical and radiographic disease activity in multiple sclerosis. Nature Communications. 2024;15:4297. PubMed
- Fox RJ, Cree BAC, de Seze J, et al. Temporal relationship between serum neurofilament light chain and radiologic disease activity in patients with multiple sclerosis. Neurology. 2024;102:e209357. PubMed
- Abdelhak A, Cerono G, Sheikhzadeh F, et al. Myelin injury precedes axonal injury and symptomatic onset in multiple sclerosis. Nature Medicine. 2025. PubMed
Leave a Reply