⏱ 8 min read
A 2026 Medicare target-trial emulation found continued levetiracetam after acute ischemic stroke was associated with 53 vs. 62 deaths per 1,000 over 90 days, a risk difference of −9 deaths per 1,000 favoring continuation.
Research Highlights
- Survival signal: continued levetiracetam after an initial month of post-stroke use was linked to 53 deaths per 1,000 vs. 62 deaths per 1,000 with discontinuation over the next 90 days.1
- Age gradient: the estimated risk difference was 0 per 1,000 at ages 66–74, −9 per 1,000 at ages 75–84, and −28 per 1,000 at age 85 or older.1
- Design strength: the researchers used target-trial emulation, a method that tries to make claims data resemble a randomized trial by defining eligibility, treatment timing, follow-up, and causal contrast before analysis.1
- Clinical calibration: the finding applies to patients already started on levetiracetam after ischemic stroke, not to blanket antiseizure-medication initiation for every stroke patient.2
- Missing tradeoffs: claims data captured deaths and prescriptions, but not seizures, electroencephalogram findings, mood changes, cognition, gait instability, falls, or quality of life.1
Acute ischemic stroke means a brain artery is blocked long enough to injure tissue. Seizures can follow stroke because injured cortex becomes electrically unstable, and antiseizure medications are often prescribed when clinicians are worried about early seizures, late post-stroke epilepsy, or recurrent events.
Levetiracetam is popular in older post-stroke patients because it has fewer drug-drug interactions than older enzyme-inducing antiseizure drugs. The tradeoff is not trivial: levetiracetam can cause irritability, mood symptoms, fatigue, cognitive complaints, and balance problems, which are exactly the domains that can already be fragile after stroke.
3,212 Older Stroke Patients Were Compared as Continuers vs. Discontinuers
Sankaranarayanan et al. used Traditional Medicare claims from 2008 through 2021 to study adults aged 66 or older who had an acute ischemic stroke, started outpatient levetiracetam within 90 days after discharge, and maintained enough initial use to enter the analysis.
The key comparison began after that initial use period. Patients were assigned to 2 practical strategies:
- Continuation: at least 1 outpatient levetiracetam dispensation of at least a 1-month supply within a 14-day grace period after time zero.
- Discontinuation: no outpatient levetiracetam prescription within that same 14-day grace period.
The short-term initial-use sample included 3,212 beneficiaries. Of those, 1,779 patients (55.4%) continued levetiracetam and 1,433 did not. Median age was 76 years, 57.6% were female, 24.4% had baseline dementia, 51.8% had diabetes, and 36.6% had depression coded in the year before stroke admission.
Target-trial emulation was the methodological center of the analysis. Instead of simply comparing people who did vs. did not refill a prescription, the researchers cloned observations, censored person-time when a clone no longer followed its assigned strategy, and used inverse-probability-of-censoring weighting. In plain English: the design tried to prevent a patient from looking artificially protected just because they had to survive long enough to receive another prescription.
90-Day Mortality Was Lower With Continued Levetiracetam
After standardization and adjustment, estimated 90-day mortality was 53 deaths per 1,000 among levetiracetam continuers vs. 62 deaths per 1,000 among discontinuers. The risk difference was −9 deaths per 1,000, with a 95% confidence interval from −12 to −5 deaths per 1,000.
Confidence interval means the range of estimates compatible with the model and sampling variation. Here, the whole interval stayed below zero, so the estimated mortality difference consistently favored continuation in the main short-term analysis.
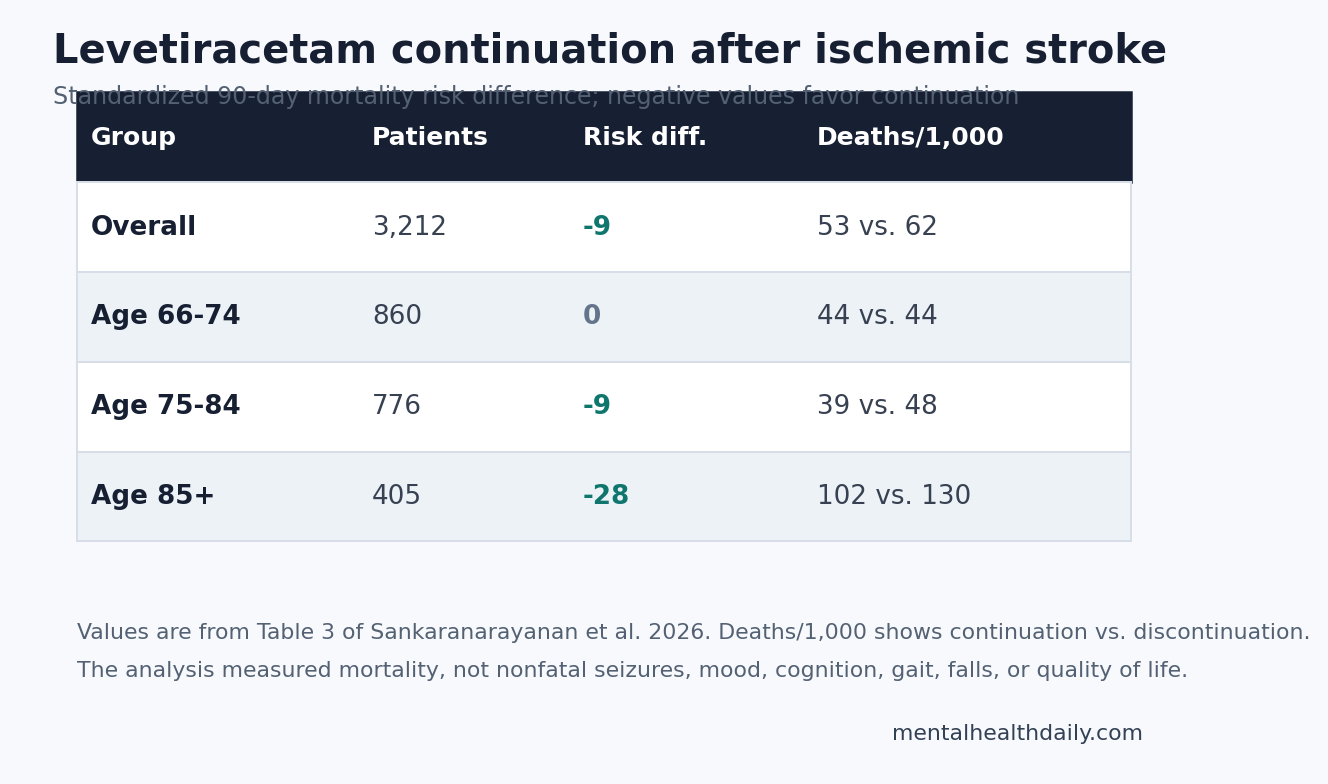
The age-stratified pattern is the useful clinical detail. Adults aged 66–74 had essentially no estimated survival difference: 0 deaths per 1,000, 95% CI −5 to +4. Adults aged 75–84 had an estimated −9 deaths per 1,000 difference, 95% CI −14 to −3. Adults aged 85 or older had the largest estimate: −28 deaths per 1,000, 95% CI −39 to −3.
That gradient keeps the result from becoming a simple “keep everyone on levetiracetam” rule. The survival signal was concentrated in older patients, while the youngest Medicare stratum did not show a clear benefit.
Continuation Is Not the Same Question as Starting Prophylaxis
The most important calibration is that Sankaranarayanan et al. studied continuation after levetiracetam had already been started. That is not the same clinical question as starting antiseizure medication in every acute ischemic stroke patient to prevent a first seizure.
Wolcott et al. reviewed antiseizure medications for primary and secondary seizure prevention after stroke and described the weak evidence base for routine long-term primary prophylaxis. Their review separated early seizures, late seizures, and post-stroke epilepsy, because recurrence risk and treatment logic differ across those groups.2
Moura et al. asked a sharper initiation question in a 2023 Stroke analysis: among adults after acute ischemic stroke, did early epilepsy-specific antiseizure-drug initiation improve short-term outcomes? Their standardized estimates did not support routine prophylaxis; estimated 30-day mortality was higher among initiators than noninitiators after adjustment.3
Sankaranarayanan et al. therefore does not erase the caution around reflexive prophylaxis. It adds a different claim: once an older patient has already started levetiracetam and sustained initial outpatient use, discontinuing vs. continuing may carry a short-term survival tradeoff, especially after age 75.
Treatment Persistence Was Already a Known Problem
Punia et al. showed why this question comes up in practice. In acute-stroke care, antiseizure medications often continue after discharge, especially when patients had clinical seizures, electrographic seizures, or epileptiform abnormalities during continuous electroencephalogram monitoring.4
Electroencephalogram monitoring records electrical activity from the scalp. It can reveal seizures or epileptiform patterns that are not obvious at bedside, which can push clinicians toward continuing medication even when the long-term plan is unclear.
Post-stroke epilepsy mortality evidence also points away from treating antiseizure medications as harmless administrative details. Larsson et al. studied antiseizure-drug monotherapy and mortality in poststroke epilepsy, emphasizing that medication choice and seizure control can be tied to survival in this population.5
The practical synthesis is narrower than either extreme:
- Starting prophylaxis broadly remains poorly supported when no seizure has occurred and no high-risk electrographic evidence is present.
- Stopping levetiracetam automatically after an older patient has already started and tolerated an initial period may be too casual, especially after age 75.
- Continuing indefinitely still needs active reassessment because this study measured mortality, not the full burden of medication harm.
Claims Data Could Not Measure the Harms Readers Care About
The survival endpoint is strong because death dates are reliably captured in Medicare data. The medication endpoint is weaker because prescription fills are not pill ingestion, and outpatient claims cannot prove why a clinician continued or stopped levetiracetam.
Several missing variables are clinically important:
- Seizure burden: the claims analysis did not capture nonfatal seizures, seizure severity, or electroencephalogram patterns.
- Stroke anatomy: lesion size, cortical involvement, and stroke mechanism were not directly measured.
- Neuropsychiatric tolerability: mood symptoms, irritability, fatigue, cognition, balance, and falls were not the primary outcomes.
- Quality of life: the analysis could not determine whether survival benefit came with better, worse, or unchanged daily function.
Schoenberg et al. is useful here because levetiracetam tolerability is not theoretical in older adults. Their randomized crossover study measured cognition, mood, and balance after levetiracetam exposure in healthy older adults, domains that post-stroke claims data can easily miss.6
Evidence-strength note: this was an observational preprint, not a completed randomized trial. Target-trial emulation improves the logic of the comparison, but it still depends on measured covariates, correct model specification, and the assumption that unmeasured prescribing factors did not drive the survival difference.
How to Read the Result Clinically
The 2026 estimate supports a middle position: levetiracetam continuation after ischemic stroke deserves a deliberate review, not reflexive stopping and not indefinite autopilot.
Age should carry weight. A 66-year-old who started levetiracetam after a small ischemic stroke, never had a seizure, has no epileptiform activity, and reports mood or balance problems is not the same patient as an 86-year-old with cortical injury, high seizure concern, and no obvious medication toxicity.
For older post-stroke patients already taking levetiracetam, the useful follow-up questions are concrete:
- Was levetiracetam started for a documented seizure, electroencephalogram abnormality, cortical stroke pattern, or vague prophylaxis?
- Has the patient had irritability, depression, sedation, gait worsening, falls, or cognitive decline since starting it?
- Is there a documented stop date, taper plan, neurology follow-up, or reason to continue through the highest-risk window?
- Does the patient fall into the older strata where the 2026 analysis found the strongest short-term survival signal?
The study’s best use is not a universal answer. It raises the bar for casual discontinuation in adults aged 75 or older who already started levetiracetam after ischemic stroke, while preserving the older warning that primary seizure prophylaxis after stroke has often outrun evidence.
Questions About Levetiracetam After Stroke
Did this study prove levetiracetam prevents death after stroke?
No. It found an adjusted association in a target-trial emulation. The design is stronger than a naive refill comparison, but it is still observational and cannot remove every unmeasured difference between patients who continued and patients who stopped.
Does this mean every stroke patient should start levetiracetam?
No. The study only included older adults who had already started outpatient levetiracetam after acute ischemic stroke and had an initial period of use. It does not support blanket primary prophylaxis for all stroke patients.
Where was the survival signal strongest?
The estimated mortality difference was strongest in adults aged 85 or older, with −28 deaths per 1,000 favoring continuation. Ages 75–84 showed −9 deaths per 1,000, while ages 66–74 showed no clear difference.
What should be monitored if levetiracetam is continued?
Mood, irritability, fatigue, cognition, balance, falls, and functional recovery deserve active monitoring. Those outcomes are central to post-stroke life but were not captured well in the Medicare claims analysis.
References
- Sankaranarayanan M, Donahue MA, Brooks JA, et al. Post-Discharge Anti-Seizure Medication Use Improves Post-Stroke Survival: An Emulated Target Trial in Older Adults. medRxiv. 2026. doi:10.64898/2026.04.17.26351149
- Wolcott ZC, Freund BE, Tatum WO, Feyissa AM. Antiseizure medications for primary and secondary seizure prevention after stroke. Front Neurol. 2025;16:1648064. doi:10.3389/fneur.2025.1648064
- Moura LMVR, Donahue MA, Yan Z, et al. Comparative effectiveness and safety of seizure prophylaxis among adults after acute ischemic stroke. Stroke. 2023;54(2):527–536. doi:10.1161/STROKEAHA.122.039946
- Punia V, Honomichl R, Chandan P, et al. Long-term continuation of anti-seizure medications after acute stroke. Ann Clin Transl Neurol. 2021;8(9):1857–1866. doi:10.1002/acn3.51440
- Larsson D, Baftiu A, Johannessen Landmark C, et al. Association between antiseizure drug monotherapy and mortality for patients with poststroke epilepsy. JAMA Neurol. 2022;79(2):169–175. doi:10.1001/jamaneurol.2021.4584
- Schoenberg MR, Rum RS, Osborn KE, Werz MA. A randomized, double-blind, placebo-controlled crossover study of the effects of levetiracetam on cognition, mood, and balance in healthy older adults. Epilepsia. 2017;58(9):1566–1574. doi:10.1111/epi.13727
Leave a Reply