⏱ 8 min read
GLP-1 receptor agonists (semaglutide, liraglutide, tirzepatide) act on the brain as well as the gut, and a 2026 real-world cohort study from Kamel-Abusalha et al. propensity-matched 118,993 GLP-1 RA users to 118,993 non-users in the TriNetX network and found a modest but statistically robust 21–23% higher hazard of new-onset hypersomnolence at 1 and 5 years.1
Research Highlights
- GLP-1 RA users had 21% higher hypersomnolence at 1 year. HR 1.21 (95% CI 1.10–1.32, p < 0.001) compared with propensity-matched non-users. Absolute risk increase: ~0.4 percentage points.1
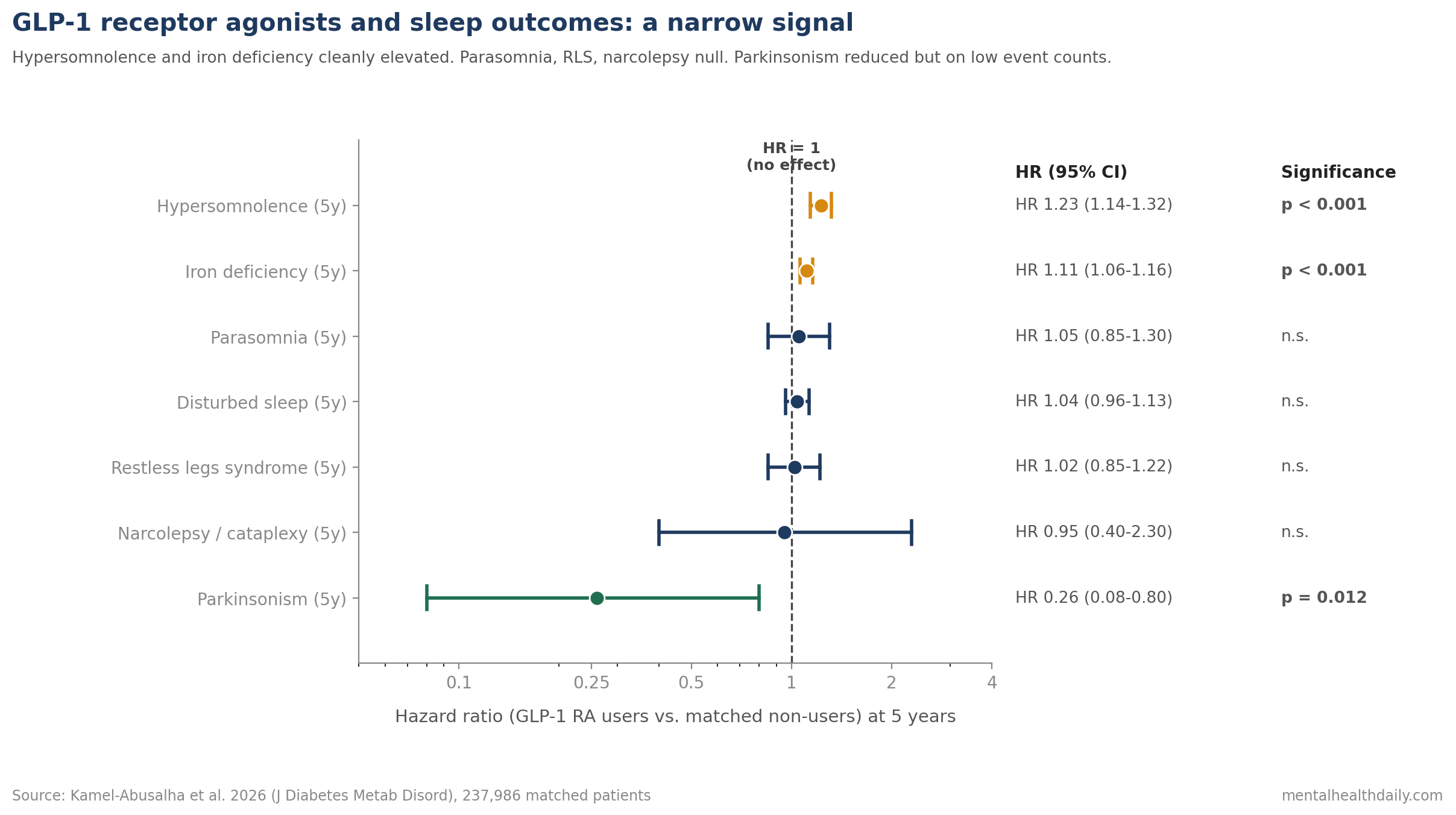
- The signal persisted at 5 years. HR 1.23 (95% CI 1.14–1.32, p < 0.001), absolute risk increase ~0.7 percentage points. The relative excess is consistent over time; the absolute excess remains small.1
- Other sleep outcomes did not move significantly. Parasomnia, disturbed sleep, restless legs syndrome, and narcolepsy/cataplexy showed no statistically significant association with GLP-1 RA exposure.1
- Iron deficiency was modestly elevated. HR 1.11 (95% CI 1.06–1.16, p < 0.001) at 5 years — consistent with known reductions in dietary intake on these drugs and worth tracking clinically.1
- Parkinsonism was reduced at 5 years, but cautiously. HR 0.26 (95% CI 0.08–0.80, p = 0.012). Event counts were low and the confidence interval is wide. The finding aligns directionally with separate trials of GLP-1 RA in Parkinson’s disease but should not be interpreted as confirmation here.1,2
GLP-1 receptors are densely expressed in the hypothalamus and brainstem — the same regions that house the orexin neurons responsible for stable wakefulness.3
The mechanistic logic for the hypersomnolence signal: GLP-1 signaling suppresses ghrelin, ghrelin normally stimulates orexin neurons in the lateral hypothalamus, and lower orexin tone produces measurable shifts in sleep–wake regulation. Preclinical data support this pathway.
Whether the signal would translate to a measurable clinical effect in real-world patients is what this analysis tested.
Kamel-Abusalha 2026: 237,986-Patient TriNetX Cohort, 1:1 Propensity Matched
The analysis used the TriNetX research network, which aggregates de-identified electronic health records from approximately 157 million patients across 107 healthcare organizations.1
Cohort selection was deliberate:
- Population: ages 18–50 with type 2 diabetes mellitus or obesity, who had undergone polysomnography (a sleep study). The polysomnography requirement enriched the cohort for documented sleep concerns and increased the chance of capturing sleep-related diagnoses in administrative data.
- Exclusion: any prior use of antidepressants, since these centrally acting agents could confound the sleep outcomes.
- Exposure: any GLP-1 receptor agonist use vs. no use.
1:1 propensity score matching balanced the two groups on demographics, comorbidities (sleep apnea, mood disorders, anxiety disorders, chronic pain), and concurrent medications (benzodiazepines, antihistamines, SGLT2 inhibitors, DPP-4 inhibitors, antihypertensives).
The matching produced 118,993 patients in each arm with standardized mean differences below 0.10 across all covariates — the conventional bar for adequate balance.
The primary outcome was new-onset hypersomnolence (ICD-10 codes G47.1 hypersomnia and R40.0 somnolence). Patients with prior history of any outcome were excluded from the analysis of that specific outcome to ensure incident-event capture.
Hypersomnolence: Modest Relative Excess, Small Absolute Excess
The hypersomnolence signal is the headline finding.
1-year hazard ratio: 1.21 (95% CI 1.10–1.32, p < 0.001). Absolute risk increase approximately 0.4 percentage points.1
5-year hazard ratio: 1.23 (95% CI 1.14–1.32, p < 0.001). Absolute risk increase approximately 0.7 percentage points.
A hazard ratio is the ratio of event rates between groups. An HR of 1.21 means GLP-1 RA users developed new hypersomnolence 21% more often than matched non-users over the follow-up window.
The 95% confidence interval is the range the true ratio likely falls in. Both intervals exclude 1.0 (no effect), making the signal statistically robust.
The absolute risk increase is more important than the relative one for individual patients. A 21–23% higher hazard sounds large; the same effect translated into absolute terms means roughly 4–7 additional cases of clinically diagnosed hypersomnolence per 1,000 patient-years of GLP-1 RA exposure.
Iron Deficiency Rose; Parasomnia, RLS, and Narcolepsy Did Not
The secondary outcomes paint a narrower picture than the abstract or pharmacovigilance reports might suggest.
Iron deficiency: HR 1.11 (95% CI 1.06–1.16, p < 0.001) at 5 years — consistent with the appetite-suppression and reduced food intake associated with these drugs. This is a real, clinically actionable signal that has been reported in trials independently of this analysis.1
Parasomnia, disturbed sleep, restless legs syndrome, narcolepsy/cataplexy: no statistically significant association with GLP-1 RA exposure in time-to-event analyses.
Parkinsonism: HR 0.26 (95% CI 0.08–0.80, p = 0.012) at 5 years. The point estimate is striking, but event counts were low and the confidence interval is wide enough that the result needs careful interpretation.
Separate randomized trials have suggested possible neuroprotective effects of GLP-1 RA in Parkinson’s disease (the lixisenatide LIX-PARK trial showed slowed motor decline at 12 months in early PD).2 The Kamel-Abusalha signal is directionally consistent with that trial but rests on a much smaller event base in a cohort that was not designed to study Parkinsonism.
Mechanism: GLP-1, Ghrelin, and the Orexin System
The mechanistic chain that connects a metabolic drug to a sleep symptom runs through the hypothalamus.
GLP-1 receptors are widely expressed in the central nervous system, with high density in the hypothalamus, brainstem, and reward-relevant regions.3
Ghrelin is a hunger-promoting hormone secreted by the stomach. Beyond its appetite role, ghrelin stimulates the orexin (also called hypocretin) neurons in the lateral hypothalamus.
Orexin neurons are the master regulators of stable wakefulness. Orexin-A and orexin-B project widely to wake-promoting regions and stabilize the sleep–wake transition. Loss of orexin signaling produces narcolepsy with cataplexy (this is the underlying biology of type 1 narcolepsy).
GLP-1 RA administration suppresses ghrelin secretion. Lower ghrelin means lower stimulation of orexin neurons. Lower orexin tone, all else being equal, predicts a modestly reduced wake-promoting drive and a tendency toward more daytime sleepiness.
The proposed pathway is consistent with the Kamel-Abusalha hypersomnolence signal, the absence of a parasomnia or RLS signal, and the directionally similar (though much weaker) parkinsonism trend — orexin signaling has documented interactions with dopamine and motor systems.
Monitor New Sleepiness and Iron Status During GLP-1 Treatment
- The hypersomnolence risk is real but small in absolute terms. Patients on semaglutide, liraglutide, or tirzepatide should be told that excessive daytime sleepiness is a possible side effect, with an absolute incidence of roughly 0.4–0.7 percentage points above baseline at 1 to 5 years.1
- Comorbid sleep disorders deserve baseline assessment. Patients with pre-existing obstructive sleep apnea, insomnia, or shift work may be more vulnerable to a sleep symptom on top of an already-stressed system. The Kamel-Abusalha cohort excluded prior history of each outcome, so the published HRs are for incident events only.
- Iron deficiency monitoring is reasonable for long-term users. The HR 1.11 signal at 5 years is small but consistent with the documented dietary changes on these drugs. Annual ferritin in patients with relevant symptoms (fatigue, hair loss, restless legs) is a low-cost intervention.
- Don’t over-read the Parkinsonism signal. The HR 0.26 estimate is striking and directionally consistent with separate trial evidence in Parkinson’s disease, but the event count is low and the cohort was not designed to test neuroprotection. Treat as hypothesis-generating, not as evidence of clinical Parkinsonism prevention.
TriNetX Diagnoses Cannot Prove GLP-1 Drugs Cause Sleepiness
It is observational. Propensity matching reduces but does not eliminate confounding. Patients prescribed GLP-1 RA may differ from those not prescribed in ways that no administrative database captures fully (motivation for weight management, clinician selection, adherence patterns).
It is a coding-based outcome. Hypersomnolence was identified by ICD-10 codes, not by polysomnography or Epworth Sleepiness Scale scores. Some patients with mild daytime sleepiness will not be coded; some patients coded for hypersomnolence may have other sleep disorders driving the symptom.
The cohort excluded antidepressant users. This sharpens the GLP-1 RA signal but limits generalizability. Many real-world GLP-1 RA users are on antidepressants, and the interaction with central agents is unaddressed here.
Drug-specific effects are not separated. GLP-1 RA was treated as a class. Whether semaglutide, liraglutide, dulaglutide, exenatide, or tirzepatide differ in their hypersomnolence association is untested in this analysis.
Dose-response was not modeled. Higher doses of semaglutide for obesity may produce different CNS effects than lower diabetes doses; the available data here do not separate them.
Questions About GLP-1 Drugs and Daytime Sleepiness
Should I be worried about feeling sleepy on Ozempic, Wegovy, or Mounjaro?
The risk is real but small in absolute terms. Roughly 4–7 additional patients per 1,000 person-years on these drugs developed clinically diagnosed hypersomnolence compared with matched non-users.1
If you experience persistent excessive daytime sleepiness on a GLP-1 RA, mention it to your prescriber. Don’t stop the drug abruptly without medical advice, especially if you’re on it for diabetes.
Why would a diabetes/weight drug cause sleepiness?
GLP-1 receptors are densely expressed in the hypothalamus and brainstem, where the orexin neurons that maintain stable wakefulness reside.3
GLP-1 RA administration suppresses ghrelin, ghrelin normally stimulates orexin neurons, and lower orexin tone produces a modest pull toward sleepiness.
Does this mean GLP-1 drugs cause narcolepsy?
No. The Kamel-Abusalha analysis specifically tested narcolepsy/cataplexy and found no significant association.1
The hypersomnolence signal is best understood as mild excess daytime sleepiness, not the severe sleep-attack pattern of narcolepsy.
Is the iron deficiency signal a real concern?
The HR 1.11 signal at 5 years is statistically robust but modest. It is consistent with reduced food intake on these drugs and aligns with reports from clinical trials.1
Annual ferritin testing is reasonable for long-term GLP-1 RA users with fatigue, restless legs, or other suggestive symptoms.
What about Parkinson’s disease — do GLP-1 drugs really protect?
The Kamel-Abusalha cohort showed a reduced Parkinsonism hazard (HR 0.26), but with low event counts and a wide confidence interval. The result is directionally consistent with the LIX-PARK randomized trial in early Parkinson’s disease but should not be read as confirmation in the general population.1,2
Separate dedicated trials are the right venue for testing neuroprotection claims.
References
- Association of GLP-1 Receptor Agonist Use with Hypersomnolence: A Real-world Cohort Analysis. Kamel-Abusalha L et al. Journal of Diabetes & Metabolic Disorders. 2026;25(1):117. doi:10.1007/s40200-026-01929-0
- Trial of Lixisenatide in Early Parkinson’s Disease. Meissner WG et al. New England Journal of Medicine. 2024;390(13):1176-1185. doi:10.1056/NEJMoa2312323
- GLP-1 receptor expression in the rat brain: detailed mapping by in situ hybridization and immunohistochemistry. Cork SC et al. Molecular Metabolism. 2015;4(10):718-731. doi:10.1016/j.molmet.2015.07.008
- The hypocretins: hypothalamus-specific peptides with neuroexcitatory activity. de Lecea L et al. Proceedings of the National Academy of Sciences. 1998;95(1):322-327. doi:10.1073/pnas.95.1.322
- Once-Weekly Semaglutide in Adults with Overweight or Obesity. Wilding JPH et al. New England Journal of Medicine. 2021;384(11):989-1002. doi:10.1056/NEJMoa2032183
Leave a Reply