
An Italian multiple sclerosis Delphi panel reached consensus on 116 of 166 votes, meaning 70% of expert votes aligned and 30% still exposed disagreement about personalized therapy, patient involvement, and treatment sequencing.1 The result supports individualized MS treatment planning, but it is consensus evidence rather than proof that one disease-modifying therapy fits every high-risk patient.
Research Highlights
- Consensus covered 70% of votes: 116 of 166 Delphi votes reached consensus, while 50 votes, or 30%, remained non-consensus.1
- Positive alignment dominated: 68% of all votes were positive-consensus votes, compared with 2% negative-consensus votes.1
- 9 experts shaped the panel: The modified Delphi process used Italian MS key opinion leaders who collectively represented major academic and specialized-care centers.1
- High-efficacy therapies led several domains: Cladribine and anti-CD20 therapies repeatedly reached 100% consensus for fewer switches, adherence, and therapeutic sequencing items.1
- Guidelines still frame the decision: ECTRIMS/EAN and AAN recommendations already support individualized disease-modifying therapy selection; this paper adds Italian expert-practice texture.2,3
Multiple sclerosis (MS) is an immune-mediated central nervous system disease in which inflammatory demyelination and neurodegeneration can produce relapses, disability accumulation, cognitive symptoms, fatigue, and sensory or motor impairment. Disease-modifying therapies (DMTs) are drugs used to reduce inflammatory activity and slow long-term disability risk, but their benefit-risk profiles differ sharply.
Personalized therapy means matching DMT choice and treatment sequence to disease activity, prognosis, comorbidities, pregnancy plans, safety risk, administration burden, access, and patient priorities. The phrase can sound vague; the Delphi paper is useful because it converts that idea into voted statements.
116 of 166 Votes Reached Consensus
Gasperini et al. used a modified Delphi design. A panel of 9 Italian MS experts developed 35 items across 8 statements and voted anonymously on domains including personalized treatment, patient participation, quality of life, caregiver burden, treatment flexibility, self-management, perceived efficacy and safety, and therapeutic sequence management.1
Delphi consensus is a structured expert-agreement method. It does not measure patient outcomes directly; it measures whether experts converge on statements after reviewing the same clinical problem.
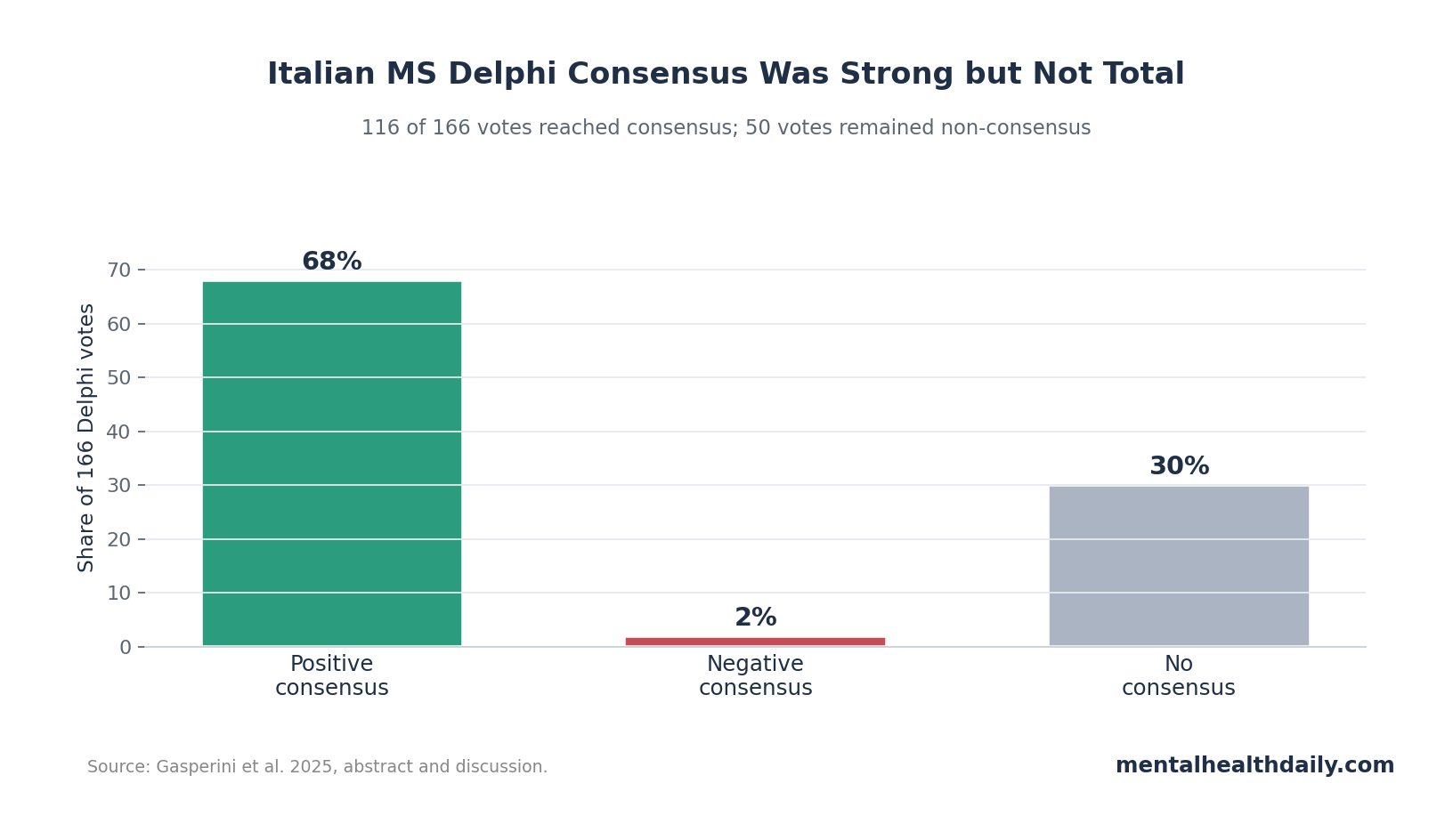
The headline count was 166 total votes: 116 reached consensus, and 50 did not. The split matters because a superficial read could turn “personalized therapy consensus” into “experts agree on everything.” They did not. The panel aligned strongly on broad principles and several high-efficacy treatment concepts, while 30% non-consensus showed that implementation still varies.
High-Efficacy DMTs Carried the Clearest Treatment Signal
The paper separated moderate-efficacy DMTs, including glatiramer acetate, interferons, dimethyl fumarate, and teriflunomide, from high-efficacy DMTs, including alemtuzumab, cladribine, fingolimod, natalizumab, ocrelizumab, ofatumumab, ozanimod, ponesimod, and siponimod.1
Cladribine and anti-CD20 therapies stood out. The panel reported 100% consensus for these therapies on fewer therapeutic switches, and high-efficacy DMTs generally received positive consensus for adherence-related and sequencing statements. Anti-CD20 therapies include drugs such as ocrelizumab and ofatumumab that deplete B cells, immune cells involved in MS inflammatory activity.
Clinical interpretation: the consensus favors early seriousness about disease control. A patient with active relapsing disease, poor prognostic markers, or breakthrough MRI activity may lose time if treatment starts with a weak option purely because it is familiar.
That does not make high-efficacy therapy automatic for every patient. Safety, infection risk, pregnancy timing, monitoring capacity, vaccine status, patient preference, and reimbursement rules can still change the decision.
Why cladribine and anti-CD20 therapies drew support: both categories can fit the practical side of MS care alongside the inflammatory-control side. Cladribine is given in short oral treatment courses, while anti-CD20 therapies such as ocrelizumab and ofatumumab use scheduled immune-cell depletion rather than daily self-administration.
In a Delphi table about flexibility, adherence, and sequencing, convenience can become part of the efficacy story because a theoretically strong drug loses value when the patient cannot stay on it.
The paper’s treatment signal should still be read as expert practice preference. A 100% consensus item means all 9 panelists agreed with that statement under the Delphi voting rule, while outcome superiority still depends on trial, registry, and safety data. That distinction matters for readers comparing MS drugs online, because consensus language can look stronger than the evidence hierarchy actually allows.
Patient Involvement Was Treated as Part of Efficacy
The Delphi statements linked communication and patient involvement to adherence, persistence, quality of life, and long-term treatment success.1 That is not soft add-on language. MS drugs only work when patients can actually stay on them, manage monitoring, tolerate administration, and understand why a therapy was chosen.
Guideline documents already emphasize counseling and shared decision-making. The ECTRIMS/EAN guideline covers pharmacological treatment choices across relapsing and progressive MS contexts, while the AAN guideline summarizes recommendations for starting, switching, and stopping disease-modifying therapies.2,3
The Italian Delphi paper adds an operational layer:
- Communication: adequate information is part of treatment selection, not a separate courtesy.
- Life plans: family planning and work-related needs were fully endorsed in treatment-sequence planning.
- Quality of life: treatment burden, caregiver burden, and disability-specific needs should influence the plan.
- Flexibility: treatment sequencing should adjust when relapse, MRI activity, tolerability, or preference changes.
The patient-involvement findings are also a reminder that MS treatment decisions happen over years, not at a single prescription visit. The PDF specifically framed flexibility around travel, work, family planning, comorbidities, parenthood, and lifestyle. Those are not peripheral preferences. They determine whether monitoring happens on time, whether a patient can manage infusion or injection schedules, and whether a pregnancy plan conflicts with the selected DMT.
Practical read: a personalized MS plan should name the tradeoff rather than hiding it. If the neurologist leans toward a high-efficacy DMT, the patient still needs a concrete explanation of infection monitoring, vaccine timing, pregnancy implications, administration schedule, and switching rules. If the plan starts with a moderate-efficacy DMT, the patient needs to know what relapse or MRI threshold would trigger escalation.
30% Non-Consensus Shows Where Personalization Gets Hard
Non-consensus is not failure in a Delphi study. It often marks the real clinical pressure points. In MS, those pressure points include how aggressively to treat early disease, how to weigh moderate safety advantages against lower efficacy, how to sequence therapies after breakthrough disease, and how to adapt national guidelines to local access rules.
Evidence hierarchy: consensus papers sit below randomized trials, comparative-effectiveness studies, and large registry analyses for determining treatment effects. Their role is different: they expose how experienced clinicians interpret a complicated evidence base when trial data do not answer every sequencing question.
Modern DMT classification work supports the broad distinction between higher- and lower-efficacy therapies, but classification is not the same as individualized prescription.4 A high-efficacy option may be biologically appropriate and still impractical if monitoring access is poor or infection risk dominates.
The single-round modified Delphi design also limits how much weight to put on the unresolved 30%. Traditional Delphi studies often use repeated rounds, feedback, and revision until panelists either converge or the disagreement becomes clearer. This paper captured expert voting across 35 items and 8 statements, but it did not show whether some non-consensus items would have shifted after another round of discussion.
That makes the non-consensus more useful as a map than as a final verdict. It points to decisions where clinicians probably need better comparative data:
- When to escalate early.
- When a lower-burden option is acceptable.
- How to sequence therapy after breakthrough disease.
- How to balance pregnancy planning against relapse risk.
- How to apply broad European or American guideline principles inside a specific health system.
Best Use Is Treatment Architecture, Not Drug Ranking
The strongest reading of this Delphi paper is architectural. MS care needs a structured treatment plan that names the disease-activity target, explains why the initial therapy fits the patient, defines when MRI or relapse activity will trigger escalation or switching, and accounts for life constraints before adherence fails.
Practical treatment architecture:
- Risk-stratify first: identify relapse pattern, MRI lesion burden, spinal-cord involvement, recovery from relapses, age, comorbidity, and pregnancy context.
- Name the treatment target: relapse control, MRI stability, disability prevention, tolerability, or administration fit should be explicit.
- Choose the DMT tier: match moderate- or high-efficacy therapy to risk, safety, and patient constraints.
- Predefine switching rules: breakthrough relapse, new MRI lesions, adverse events, or adherence failure should trigger a planned response.
This is where consensus can help: it turns “personalized medicine” into a checklist of decisions that should not be left vague.
For clinicians, the most defensible use is to make the treatment plan auditable. The chart should explain why the chosen DMT fits the patient’s current inflammatory risk, what safety monitoring is required, what life constraints were considered, and what event would trigger a switch.
For patients, the useful question is not “which drug won the Delphi panel?” It is whether the treatment plan has a clear reason, a clear monitoring schedule, and a clear next step if disease activity continues.
Questions About Personalized MS Therapy
Does this Delphi paper prove high-efficacy therapy is better for everyone with MS?
No. It shows expert consensus around high-efficacy therapies in several treatment-planning domains. Trial and registry evidence still determine comparative benefits and risks for specific patient groups.
Why did cladribine and anti-CD20 therapies stand out?
The panel viewed them as effective and convenient enough to support fewer switches, adherence, and sequencing confidence. The paper also noted that interpretation varied for some safety and tolerability statements, so the signal should be read as expert preference within context.
What should patients take from this?
The useful takeaway is not to demand a specific drug from a consensus table. It is to ask whether the treatment plan clearly explains risk level, DMT rationale, monitoring, switching triggers, pregnancy or life constraints, and expected adherence burden.
References
- Gasperini C, Centonze D, Conte A, et al. Personalized therapy in multiple sclerosis: an Italian Delphi consensus. Journal of Neurology. 2025;272:428. doi:10.1007/s00415-025-13173-2
- Montalban X, Gold R, Thompson AJ, et al. ECTRIMS/EAN guideline on the pharmacological treatment of people with multiple sclerosis. Multiple Sclerosis Journal. 2018;24(2):96-120. doi:10.1177/1352458517751049
- Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: disease-modifying therapies for adults with multiple sclerosis. Neurology. 2018;90(17):777-788. doi:10.1212/wnl.0000000000005347
- Samjoo IA, Worthington E, Drudge C, Zhao M, Cameron C, Haring DA, et al. Efficacy classification of modern therapies in multiple sclerosis. Journal of Comparative Effectiveness Research. 2021;10(6):495-507. doi:10.2217/cer-2020-0267
- Ontaneda D, Tallantyre EC, Raza PC, et al. Determining the effectiveness of early intensive versus escalation approaches for the treatment of relapsing-remitting multiple sclerosis: the DELIVER-MS study protocol. Contemporary Clinical Trials. 2020;95:106009. doi:10.1016/j.cct.2020.106009
Leave a Reply