⏱ 8 min read
A 2026 cross-sectional study of 519 older adults with first-episode depression found that the NOS3 rs1799983 TT genotype was independently associated with cognitive impairment, adjusted OR 1.720 (95% CI 1.027-2.882).1 The result is strongest as a vascular-inflammation clue, not as a ready clinical genetic test.
Research Highlights
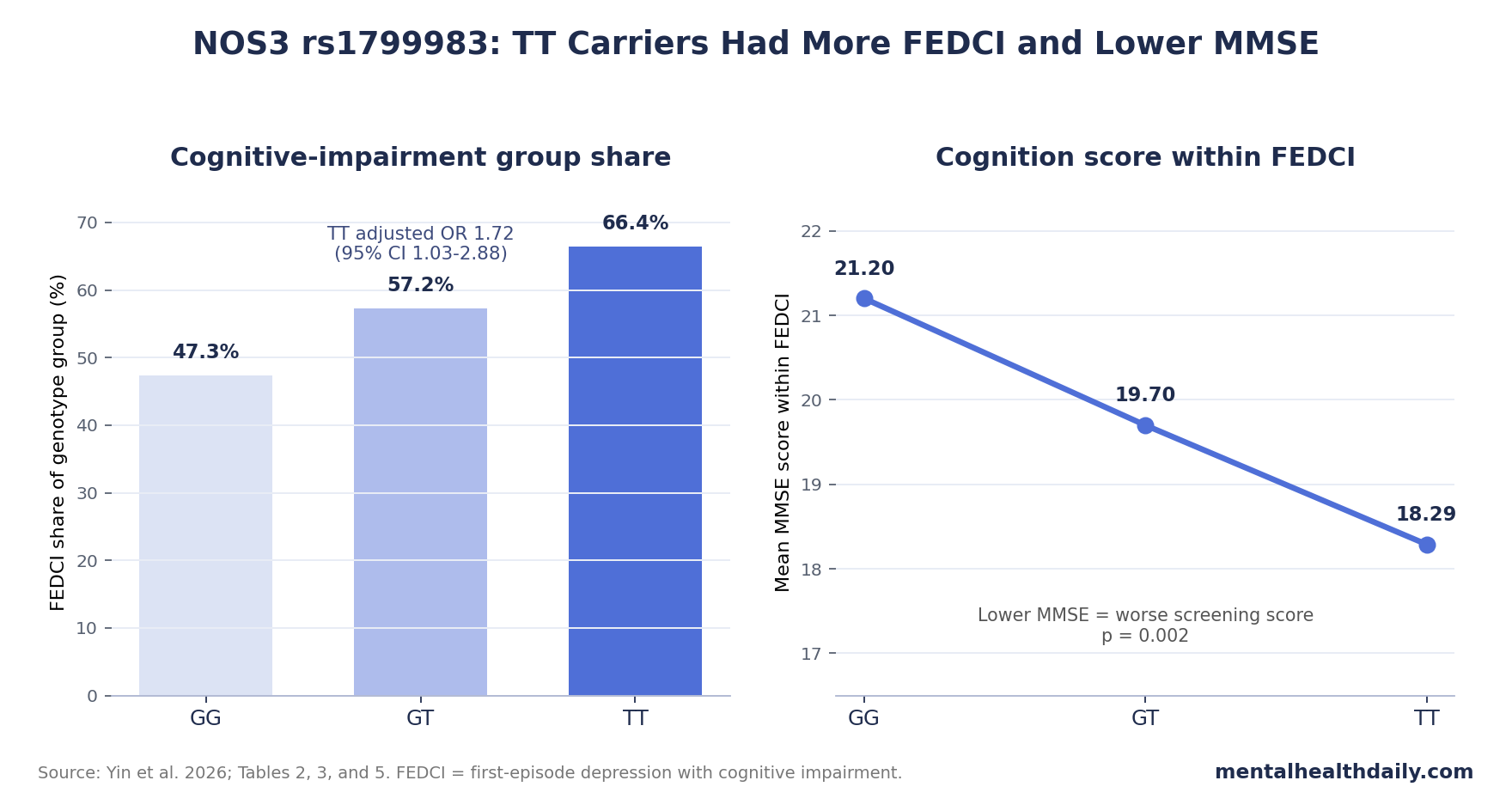
- TT genotype carried the headline signal: in multivariable modeling, NOS3 rs1799983 TT was associated with first-episode depression plus cognitive impairment, OR 1.720 (95% CI 1.027-2.882, p = 0.039).1
- Genotype frequencies leaned in the same direction: TT appeared in 17.86% of depression-only patients vs. 26.78% of patients with depression and cognitive impairment.1
- Cognition tracked genotype inside FEDCI: Mini-Mental State Examination scores averaged 21.20 for GG, 19.70 for GT, and 18.29 for TT carriers.1
- Inflammation moved opposite NOS3: TNF-α, IL-1β, and IL-6 were all higher in the cognitive-impairment group, while NOS3 expression was lower and positively correlated with MMSE score.1
- Evidence strength stays limited: the study was cross-sectional and single-center, so it can support risk-marker biology in 519 patients but not causality or stand-alone genetic screening.1
NOS3 is the gene for endothelial nitric oxide synthase, an enzyme that helps blood-vessel lining cells produce nitric oxide, a signaling molecule involved in blood-flow regulation, endothelial stability, and inflammatory control. The rs1799983 variant is also called G894T or Glu298Asp; the shorthand means a single-letter DNA change that can alter the amino-acid sequence of the enzyme.
Yin et al. studied 224 patients with first-episode depression without cognitive impairment and 295 patients with first-episode depression with cognitive impairment (FEDCI). Cognitive impairment was classified with education-adjusted Mini-Mental State Examination (MMSE) thresholds: 18 for illiterate patients, 21 for 1-6 years of education, and 25 for more than 7 years of education.1
NOS3 TT Carriers Had Higher Cognitive-Impairment Odds
The central result came from logistic regression. After adjustment, lower MMSE score, lower NOS3 expression, and the rs1799983 TT genotype remained associated with FEDCI. The TT genotype carried OR 1.720 (95% CI 1.027-2.882, p = 0.039). Higher NOS3 expression moved in the opposite direction, OR 0.577 (95% CI 0.375-0.889, p = 0.013), meaning higher measured expression was associated with lower odds of being in the cognitive-impairment group.1
Genotype distribution: TT was not rare in either group, but it was more concentrated in FEDCI. The depression-only group had 69 GG, 115 GT, and 40 TT patients. The FEDCI group had 62 GG, 154 GT, and 79 TT patients. In pooled sample terms, the share classified as FEDCI rose from 47.3% among GG carriers to 57.2% among GT carriers and 66.4% among TT carriers.
Clinical translation: the TT result is a risk-marker association, not a deterministic claim. Many TT carriers in this sample were not cognitively impaired, and many cognitively impaired patients were not TT carriers. The value is that the genotype points toward a biological pathway worth testing: endothelial nitric oxide signaling, inflammation, and vascular contribution to cognition.
MMSE Scores Were Lowest in TT Carriers With FEDCI
Inside the FEDCI group, average MMSE scores separated by genotype: 21.20 for GG, 19.70 for GT, and 18.29 for TT, with p = 0.002 for the reported genotype comparison.1 The same genotype split did not meaningfully separate MMSE scores inside the depression-only group, where averages were 22.93, 22.94, and 22.44.
That pattern makes the association more specific. The TT genotype showed its clearest separation in the subgroup already meeting cognitive-impairment criteria, where TT carriers also had lower NOS3 expression and higher inflammatory-marker expression.
MMSE limitation: MMSE is a screening tool, not a full neuropsychological battery. It is useful for broad cognitive classification in older adults, but it does not map memory, processing speed, executive function, language, and attention with the precision needed to define a cognitive phenotype. A future replication should use deeper cognitive testing before treating this as a domain-specific deficit.
Inflammatory Markers Pointed Away From Higher NOS3 Expression
Yin et al. measured serum NOS3 and 3 inflammatory markers by RT-qPCR: tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), and interleukin-6 (IL-6). All 3 inflammatory markers were higher in FEDCI than in depression without cognitive impairment, each with p < 0.001 in the figures.1
NOS3 expression moved in the opposite direction. The FEDCI group had lower NOS3 expression, and NOS3 expression was negatively correlated with TNF-α, IL-1β, and IL-6. NOS3 expression was also positively correlated with MMSE score, which means higher expression tracked less severe cognitive impairment in this sample.
Mechanistic read: endothelial nitric oxide synthase can support vascular tone and endothelial function, while nitric oxide signaling can interact with inflammatory pathways such as NF-κB. The study does not prove that a lower NOS3 signal caused inflammation in the brain, but the peripheral pattern fits a plausible vascular-inflammatory route into late-life depression cognition.
Depression-Cognition Evidence Already Supports the Target
The broader literature makes the target credible before the gene result enters the picture. Rock et al. reviewed cognitive impairment in depression and found that cognitive deficits are not peripheral complaints; memory, attention, and executive-function problems are repeatedly measurable in depressed patients.2 That background supports studying cognition in first-episode depression instead of treating it as an unrelated aging problem.
Longitudinal older-adult data also point in the same direction. The LADIS study reported that depressive symptoms predicted cognitive decline and dementia in older people independently of cerebral white matter changes.3 That does not make depression a simple cause of dementia, but it does mean depression and cognitive decline can travel together even after visible small-vessel disease is considered.
NOS3 is a narrower candidate inside that larger map. Manso-Calderon et al. analyzed endothelial-pathway polymorphisms in vascular dementia and Alzheimer’s disease, including NOS3 variation.4
Wang et al. also reported that the same G894T/rs1799983 variant was associated with ischemic stroke risk across 22 studies, including dominant, recessive, and codominant models.5 Those papers do not validate the Yin result directly, but they keep the variant inside a vascular-brain-risk neighborhood rather than making it a random candidate-gene hit.
Cross-Sectional Genetics Cannot Prove a Clinical Test
The strongest caution is design. This was a cross-sectional, single-center study. The researchers measured genotype, serum expression, inflammatory markers, depression severity, and cognitive status at one broad time point. That design can show that variables cluster together, but it cannot show whether TT genotype caused lower NOS3 expression, whether inflammation preceded cognitive impairment, or whether cognitive impairment preceded more severe depressive symptoms.
Several additional limits keep the result preliminary:
- Ancestry and setting: the sample came from one Chinese hospital system, so effect size and allele-frequency estimates may differ in other populations.
- Peripheral measurement: serum RT-qPCR expression is not a direct measurement of brain endothelial nitric oxide signaling.
- Phenotype depth: MMSE is too coarse to identify which cognitive systems are most affected.
- Table-label inconsistency: Table 5 appears to label the genotype term as rs9588884 even though the paper text and surrounding tables discuss rs1799983; the surrounding context points to rs1799983, but the inconsistency should be fixed in any future citation or replication.
The useful next test is not direct-to-consumer NOS3 screening for depression patients. It is replication in larger, multi-ancestry cohorts with longitudinal follow-up, medication data, vascular-risk measurement, full cognitive batteries, and inflammatory/endothelial biomarkers measured over time.
For current care, the safer clinical implication is broader than genetics. Older adults with first-episode depression and low cognitive screening scores need a workup that treats cognition, vascular risk, inflammation, sleep, medication effects, and mood severity as interacting problems. A candidate-gene association can help frame that biology, but it should not displace basic clinical evaluation.
The study also argues for better phenotype labels. “Depression with cognitive impairment” can mean slow processing speed, memory encoding problems, executive dysfunction, low effort from severe mood symptoms, early neurodegenerative disease, vascular cognitive impairment, or a mixture of those patterns. If future NOS3 studies keep using only broad MMSE cutoffs, they may reproduce a risk signal without learning which cognitive system is actually linked to endothelial nitric oxide biology.
A useful replication would therefore separate memory, attention, executive function, processing speed, vascular burden, and inflammatory profile before testing genotype. That design would show whether NOS3 rs1799983 marks a specific vascular-cognitive pathway or only tracks a broad high-risk depression subgroup.
Questions About NOS3 and Depression-Related Cognition
Does this mean the NOS3 TT genotype causes cognitive impairment in depression?
No. The study found an adjusted association in a cross-sectional sample. Causality would require longitudinal evidence showing that genotype-linked NOS3 biology precedes cognitive decline and cannot be explained by education, vascular disease, inflammation, depression severity, medication exposure, or other confounders.
Should older adults with depression be genotyped for NOS3 rs1799983?
Not from this evidence alone. A single OR 1.720 association is not enough for clinical genotyping, especially when the phenotype was measured with MMSE and the sample came from one center.
What should clinicians or researchers take from the result?
The practical research lead is vascular-inflammatory phenotyping. In older adults with first-episode depression, cognitive screening should be paired with vascular risk, inflammatory markers, and more detailed neuropsychological testing before anyone treats a candidate gene as a clinical decision tool.
References
- Yin Y, Tang L, Xia J, et al. Association of NOS3 rs1799983 Polymorphism with Cognitive Function in Patients with First Episode Depression. Clinical Psychopharmacology and Neuroscience. 2026;24(2):368-378. doi:10.9758/cpn.25.1361
- Rock PL, Roiser JP, Riedel WJ, Blackwell AD. Cognitive impairment in depression: a systematic review and meta-analysis. Psychological Medicine. 2014;44(10):2029-2040. doi:10.1017/s0033291713002535
- Verdelho A, Madureira S, Moleiro C, et al. Depressive symptoms predict cognitive decline and dementia in older people independently of cerebral white matter changes: the LADIS study. Journal of Neurology, Neurosurgery & Psychiatry. 2013;84(11):1250-1254. doi:10.1136/jnnp-2012-304191
- Manso-Calderon R, Cacabelos-Perez P, Sevillano-Garcia MD, Herrero-Prieto ME, Gonzalez-Sarmiento R. Analysis of endothelial gene polymorphisms in Spanish patients with vascular dementia and Alzheimer’s disease. Scientific Reports. 2023;13:13441. doi:10.1038/s41598-023-39576-7
- Wang M, Jiang X, Wu W, Zhang D. Association of G894T polymorphism in endothelial nitric oxide synthase gene with the risk of ischemic stroke: a meta-analysis. Biomedical Reports. 2013;1(1):144-150. doi:10.3892/br.2012.23
Leave a Reply