
⏱ 8 min read
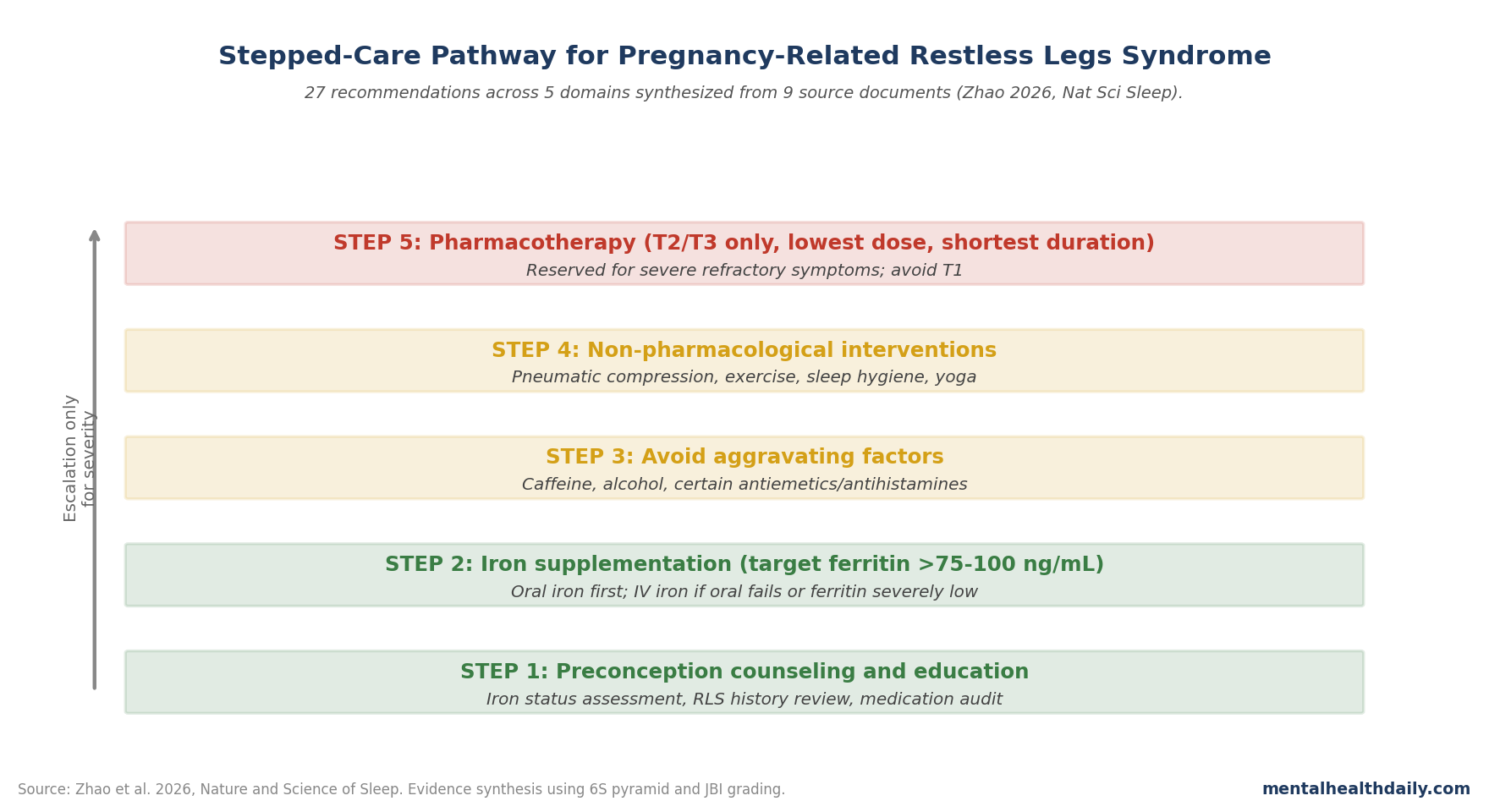
Restless legs syndrome (RLS), now also called Willis-Ekbom disease (WED), is a sleep-disrupting neurologic disorder that affects roughly 20–30% of pregnancies in some series and is linked to preeclampsia, increased cesarean delivery, and perinatal depression. A 2026 Nature and Science of Sleep synthesis turned 9 source documents into 27 practice recommendations across 5 domains, ending in a stepped-care pathway from preconception counseling to tightly restricted pharmacotherapy.1
Research Highlights
- Methodology: 6S evidence pyramid retrieval; JBI Grading of Evidence and Recommendation System.
- Sources: 9 documents synthesized into 27 practice recommendations.
- 5 domains: Aggravating factors, preconception counseling, iron supplementation, non-pharmacological treatment, pharmacological treatment.
- Stepped care: Prevention → iron + non-pharm → pharm reserved for severe refractory cases in T2/T3 only.
- 3 maternal risks: Preeclampsia, increased cesarean delivery, and perinatal depression are the major adverse-outcome signals.
- Iron is central: Ferritin and transferrin saturation testing guide repletion, with many RLS recommendations aiming above 75–100 ng/mL.
Why Pregnancy RLS Is a Distinct Clinical Problem
RLS in pregnancy differs from general-population RLS in several important ways.2
- Onset and trajectory: many women experience RLS for the first time during pregnancy, with peak severity in the third trimester and resolution within weeks of delivery.
- Pharmacological constraints: first-line RLS medications — dopamine agonists like pramipexole and ropinirole, alpha-2-delta calcium-channel ligands like gabapentin — have pregnancy-safety concerns that limit their use.
- Iron physiology: pregnancy creates substantial iron demand, and iron deficiency is one of the strongest mechanistic drivers of RLS symptoms.
Untreated pregnancy RLS carries real maternal harm. The sleep disruption alone is substantial: women with severe pregnancy RLS often lose 1–3 hours of sleep nightly. The downstream consequences include increased risk of preeclampsia, gestational hypertension, cesarean delivery, and perinatal depression. The depression risk in particular has emerged as a major reason to prioritize active management rather than dismissing pregnancy RLS as “temporary.”
The Iron Story Is the Foundation
Brain iron deficiency is one of the best-established mechanisms in RLS pathophysiology. Iron is essential for tyrosine hydroxylase function in dopamine synthesis; brain iron deficiency disrupts striatal dopamine signaling in patterns that produce the characteristic RLS symptom profile. Pregnancy creates substantial whole-body iron demand to support fetal development and increased maternal blood volume, and iron deficiency — clinical or subclinical — is common.3
The synthesis recommendations make iron assessment and repletion central to pregnancy RLS management. Specifically: serum ferritin and transferrin saturation testing should occur in pregnant women with RLS symptoms; oral iron supplementation should target ferritin above 75–100 ng/mL, which is higher than the threshold used for general-population iron supplementation; intravenous iron is appropriate when oral iron fails, isn’t tolerated, or when ferritin is severely low.
This is one of the few interventions where the evidence-pregnancy fit is straightforward: iron is needed regardless of pregnancy, the maternal-fetal benefit profile is favorable, and the mechanistic case for RLS-specific benefit is strong.
Non-Pharmacological Measures Before Drugs
The stepped-care framework places non-pharmacological measures squarely between iron repletion and pharmacotherapy. Several interventions have evidence support for RLS in general populations and reasonable safety profiles for pregnancy:
- Pneumatic compression devices. Sequential leg compression has RCT evidence for RLS symptom reduction and is essentially side-effect-free.
- Moderate exercise. Regular aerobic and resistance exercise reduces RLS severity in non-pregnant populations; pregnancy-appropriate adaptations apply.
- Sleep hygiene and timing. Consistent bedtime, avoidance of late-evening stimulants, and bedroom environment optimization help with the sleep-disruption component.
- Avoidance of aggravating substances. Caffeine, alcohol, and certain medications (including some antiemetics and antihistamines) can worsen RLS; review and adjustment is part of standard management.
- Yoga and mindfulness-based interventions. Smaller evidence base but reasonable safety; helpful for the comorbid sleep disturbance and stress.
The integrated framework treats these as a layered approach rather than alternatives — iron repletion plus exercise plus hygiene measures together, escalating to pharmacological therapy only when severity persists despite the foundational interventions.
Pharmacotherapy: Last Resort, Specific Restrictions
The synthesized recommendations restrict pharmacotherapy to severe refractory cases, in the second or third trimester only, at the lowest effective dose for the shortest necessary duration. First trimester pharmacotherapy is generally avoided because of organogenesis sensitivity and limited pregnancy-specific safety data.1
Drug-specific considerations: dopamine agonists (pramipexole, ropinirole) have limited pregnancy data and are generally avoided. Levodopa has more clinical experience and may be considered short-term. Alpha-2-delta ligands (gabapentin) are sometimes used in third trimester for severe symptoms, with attention to neonatal withdrawal monitoring. Opioids are reserved for the most severe refractory cases given dependence and neonatal abstinence considerations.
The shortest-duration principle is the key feature. Many pregnancy RLS cases resolve within weeks postpartum; if pharmacotherapy is initiated late in pregnancy for severe symptoms, plans for postpartum reassessment and discontinuation are part of the care plan rather than indefinite continuation.
The Preconception Window Is Often Missed
One of the synthesis recommendations the authors emphasize: women with pre-pregnancy RLS or known iron deficiency benefit from preconception evaluation and iron optimization before pregnancy begins. This is a clinical contact point that’s often missed because RLS is treated symptomatically by general practitioners or self-managed without specialist input.1
For a woman with established RLS planning pregnancy, the preconception window allows iron repletion to a target ferritin level, review of any RLS medications for pregnancy compatibility, and counseling about expected pregnancy trajectory. This proactive approach reduces the likelihood of severe third-trimester RLS requiring last-resort pharmacotherapy.
The Perinatal Depression Connection
Pregnancy RLS is associated with elevated perinatal depression risk, and the relationship is bidirectional. RLS’s sleep-disrupting effects amplify depression risk; depression in turn worsens subjective RLS severity. Active RLS management may be perinatal depression prevention in patients with severe symptoms.4
This connection argues against a watchful-waiting approach to severe pregnancy RLS. The temptation to dismiss pregnancy RLS as a temporary nuisance ignores the documented downstream maternal psychiatric burden when severe symptoms persist for weeks or months.
Pregnancy RLS Evidence Still Relies on Extrapolation
The Zhao synthesis is constrained by source-document availability. Pregnancy RLS has been understudied relative to general-population RLS; high-quality randomized trials in pregnancy are rare, and many recommendations are extrapolated from non-pregnant populations or based on expert consensus.1
Specific gaps include: limited comparative data on intravenous iron formulations in pregnancy; uncertainty about optimal ferritin targets for RLS-specific benefit; thin evidence on third-trimester gabapentin safety beyond neonatal withdrawal; and lack of direct evidence on whether active RLS management reduces preeclampsia or cesarean rates.
Pathway logic: mild symptoms can start with sleep scheduling, trigger review, compression or stretching strategies, and iron workup rather than medication.
Severe symptoms should not be dismissed, but the escalation logic stays narrow: correct iron deficiency first, remove aggravating drugs or caffeine when possible, and reserve dopamine agonists, gabapentin-type drugs, or opioids for carefully selected cases where maternal sleep loss and distress outweigh medication uncertainty.
That sequence also keeps obstetric and psychiatric care connected. Pregnancy RLS can look like ordinary insomnia until clinicians ask about the urge to move, evening worsening, relief with movement, and recurrence after rest. When those features are present, documenting ferritin, depression symptoms, sleep disruption, and gestational timing helps distinguish a transient nuisance from a syndrome that may need stepped follow-up before delivery and after birth.
Iron status is the clearest example of why a pathway matters. A patient can have a hemoglobin value that looks acceptable while ferritin is still low enough to worsen RLS symptoms.
The stepped-care recommendation therefore treats ferritin and iron repletion as a neurologic-sleep intervention as well as an anemia screen. That framing helps avoid 2 errors: giving sedating drugs before correcting an obvious contributor, and ignoring severe symptoms because pregnancy is temporary.
Medication review: pregnancy care also needs a trigger audit. Antihistamines, dopamine-blocking antiemetics, some antidepressants, caffeine, and untreated iron deficiency can worsen restless legs symptoms in susceptible patients. A stepped pathway makes those contributors visible before the visit jumps to a new sleep drug.
The pathway also creates a postpartum checkpoint. Most pregnancy-onset RLS improves after delivery, but persistent symptoms should prompt reassessment of iron stores, medication exposures, sleep disruption, mood symptoms, and family history. That follow-up prevents a pregnancy-limited syndrome from becoming an untracked chronic sleep problem.
Questions About RLS in Pregnancy
How common is pregnancy RLS?
Estimates vary widely — 10–30% in different cohorts — with peak prevalence and severity in the third trimester. Many women experience RLS for the first time during pregnancy.
Will my pregnancy RLS go away after delivery?
For most women, yes — symptoms resolve or substantially improve within weeks postpartum. A subset develops chronic RLS that persists or recurs.
Is iron supplementation safe in pregnancy?
Yes, and it’s often necessary regardless of RLS. Standard prenatal vitamins contain iron; additional supplementation should be guided by ferritin testing and clinical judgment.
Can I exercise if I have pregnancy RLS?
Generally yes, and exercise often helps. Standard pregnancy exercise guidelines apply: avoid contact sports and exercises with fall risk; moderate aerobic and resistance exercise is appropriate for most women.
What about restless legs at night specifically?
Sleep-onset and middle-of-night RLS is the most common presentation. Stimulus-control approaches, leg massage, warm baths before bed, and pneumatic compression are reasonable first measures alongside iron optimization.
References
- Zhao FY et al. Development of a stepped-care pathway for managing Willis-Ekbom disease/restless legs syndrome during pregnancy: a best evidence synthesis. Nat Sci Sleep. 2026;18:591-616. doi:10.2147/nss.s591116
- Picchietti DL et al. Consensus clinical practice guidelines for the diagnosis and treatment of restless legs syndrome/Willis-Ekbom disease during pregnancy and lactation. Sleep Med Rev. 2015;22:64-77. doi:10.1016/j.smrv.2014.10.009
- Allen RP, Earley CJ. The role of iron in restless legs syndrome. Mov Disord. 2007;22(S18):S440-S448. doi:10.1002/mds.21607
- Wesstrom J et al. Pregnancy and restless legs syndrome: a population-based study. Sleep Med. 2010;11:1186-1191. doi:10.1016/j.sleep.2009.09.007
- Garcia-Borreguero D et al. Guidelines for the first-line treatment of restless legs syndrome/Willis-Ekbom disease, prevention and treatment of dopaminergic augmentation: a combined task force of the IRLSSG, EURLSSG, and the RLS-foundation. Sleep Med. 2016;21:1-11. doi:10.1016/j.sleep.2016.01.017
Leave a Reply