
⏱ 9 min read
A 2026 randomized trial in early postmenopausal women found that 8 weeks of app-based combined aerobic and resistance exercise reduced Beck Depression Inventory scores by 7.30 points, compared with 2.20 points after education-only control and 5.65 points after face-to-face exercise. A structured home program delivered through a mobile platform improved depression, fatigue, sleep quality, and menopause symptoms when adherence barriers made in-person sessions hard to attend, while still leaving supervision and adherence questions open.
Research Highlights
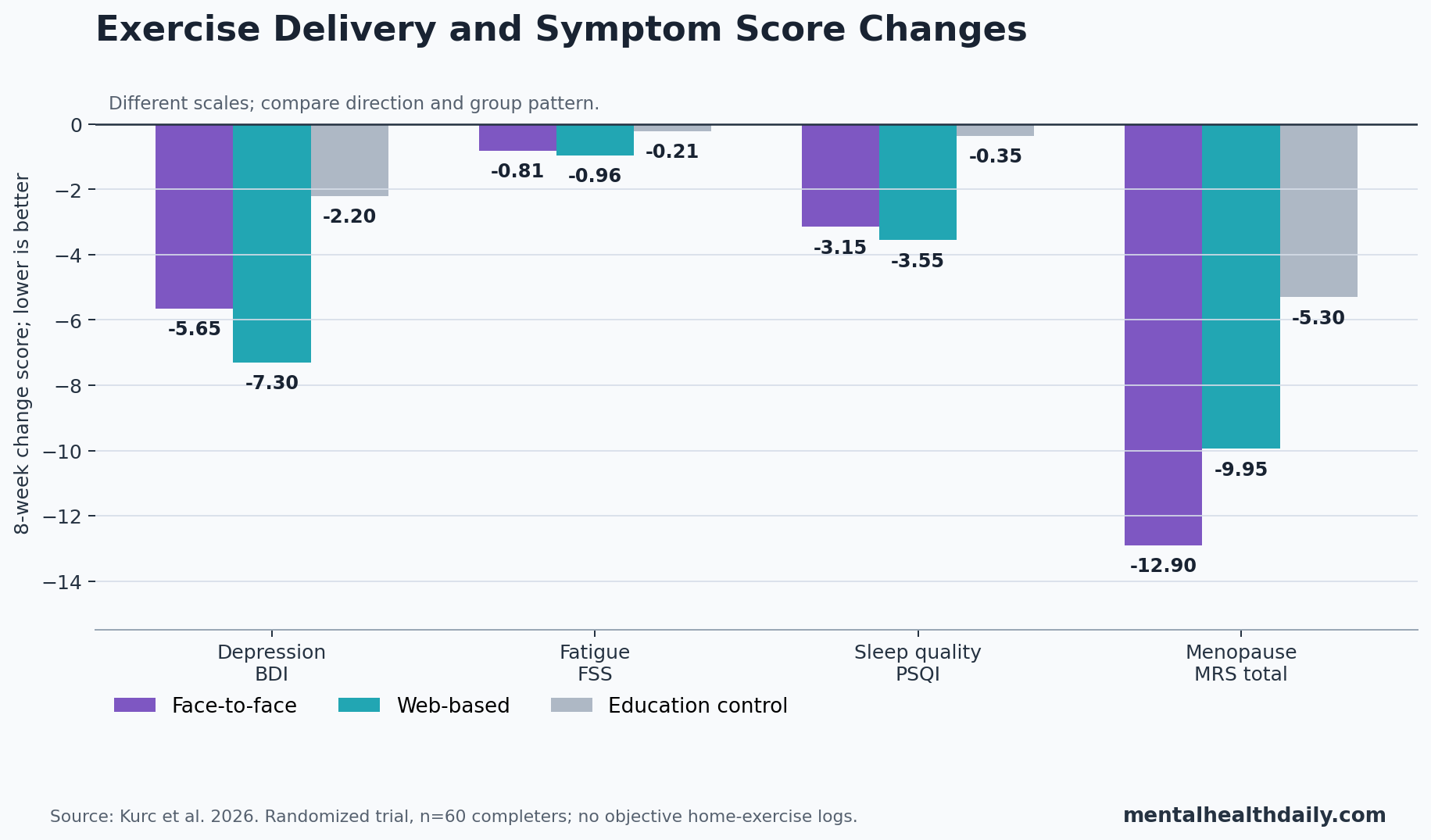
- Depression scores fell most in the app group: Beck Depression Inventory scores changed by −7.30 points with web-based exercise, −5.65 with face-to-face exercise, and −2.20 with education control.
- Menopause symptoms improved in both exercise arms: Menopause Rating Scale total scores fell by −12.90 points with face-to-face exercise and −9.95 with web-based exercise vs. −5.30 with education control.
- Fatigue and sleep moved together: fatigue showed large exercise effects vs. control (d = −1.04 to −1.66), and Pittsburgh Sleep Quality Index effects were also large (d = −1.08 to −1.19).
- Delivery differences were small: most face-to-face vs. web-based effect sizes were negligible to small, including depression (d = 0.28), fatigue (d = 0.20), and sleep quality (d = 0.15).
- Adherence is the weak link: all face-to-face participants attended 4 supervised sessions, but home exercise logs were not collected and app usage records were unavailable after the study period.
Web-based exercise means a structured physical-therapy-style program delivered through a phone app with video demonstrations, written instructions, and reminders. In this trial, it was not a casual wellness app: the web-based group received the same 8-week exercise prescription as the face-to-face group.
Early postmenopause refers to the first years after the final menstrual period, when estrogen has fallen and symptoms such as hot flashes, sleep problems, fatigue, mood changes, body-composition shifts, and lower quality of life can cluster. Exercise is attractive in that window because it targets several parts of the cluster at once, but the evidence has been uneven and attendance barriers are real.
60 Women Completed an 8-Week Exercise or Education Program
Kurc et al. randomized 66 early postmenopausal women aged 45–60 years into 3 groups: face-to-face supervised exercise, web-based exercise through PhysiApp, or education-only control. Six women withdrew before receiving the intervention, leaving 60 completers, with 20 women in each arm.
Both exercise groups followed an identical home-based program 3 days per week on nonconsecutive days. The protocol combined brisk walking, resistance exercises, core stabilization, and balance work. The face-to-face group met a physiotherapist at weeks 0, 2, 4, and 6 for demonstration, technique correction, and progression. The web-based group received video demonstrations, Turkish written instructions, audio cues, and automated reminders through the app.
Education control: women received an illustrated menopause brochure but no structured exercise program or additional supervision. Outcomes were measured at baseline and week 8 by an assessor blinded to group assignment.
Evidence-strength note: this was a small, single-region randomized trial with self-reported psychological and symptom outcomes. Randomization improves causal inference, but the trial cannot prove long-term maintenance, cannot show that the app and supervised groups completed the same exercise dose, and should not be read as treatment evidence for diagnosed major depressive disorder.
Web-Based Exercise Produced the Clearest Depression Result
Beck Depression Inventory (BDI) scores measure depressive-symptom burden over the prior 2 weeks; lower scores mean fewer symptoms. Baseline BDI scores were in the mild-to-moderate range on average: 16.00 in the face-to-face group, 19.00 in the web-based group, and 15.65 in the control group.
After 8 weeks, the web-based exercise group improved by 7.30 BDI points, and the difference vs. education control survived Bonferroni correction (p = 0.002). Face-to-face exercise improved by 5.65 points within group (p = 0.002), but the face-to-face vs. control comparison did not pass the trial’s corrected post-hoc threshold.
That pattern should be read carefully. The result does not show that app-based exercise is inherently better than supervised exercise for mood. The between-delivery effect size for BDI was small (d = 0.28), and the face-to-face arm still moved in the favorable direction. The stronger claim is narrower: in this small trial, the web-based arm produced the most statistically secure depression-score improvement vs. education control.
Sleep and Fatigue Improved in Both Exercise Arms
Fatigue Severity Scale (FSS) scores measure how much fatigue interferes with daily function; lower scores are better. Fatigue decreased by 0.81 points with face-to-face exercise, 0.96 points with web-based exercise, and 0.21 points with education control. Both exercise groups beat control after correction, with large effect sizes vs. control.
Pittsburgh Sleep Quality Index (PSQI) scores measure subjective sleep quality over the prior month; lower scores indicate better sleep. PSQI scores improved by 3.15 points in the face-to-face group and 3.55 points in the web-based group, compared with 0.35 points in the control group. Both exercise arms beat control at p = 0.001.
The sleep-fatigue-depression cluster is clinically plausible. Baker et al. reviewed evidence that sleep problems during the menopausal transition often interact with hot flashes, insomnia symptoms, mood, and daytime functioning. In Kurc et al., fatigue and sleep improved alongside BDI scores, which fits the idea that exercise may help the symptom cluster rather than a single isolated endpoint.
Menopause Symptoms Improved More Than Education Alone
Menopause Rating Scale (MRS) scores summarize symptom burden across somatic-vegetative symptoms, psychological symptoms, and urogenital symptoms. Total scores fell by 12.90 points in the face-to-face group, 9.95 points in the web-based group, and 5.30 points in the education-only group.
Both exercise arms improved more than control on total MRS score and on somatic, psychological, and urogenital subscales. Face-to-face exercise had the larger total MRS effect vs. control (d = −1.16) than web-based exercise (d = −0.76), and face-to-face exercise also produced a larger urogenital-score change than web-based exercise.
Adjacent evidence keeps the result calibrated. Money et al. reviewed 17 systematic reviews covering 80 unique primary studies and 8,983 participants. They found some support for yoga and, to a lesser extent, aerobic exercise, but concluded that evidence was still insufficient to recommend one specific exercise form for menopause symptoms.
Yilmaz Babacan et al. later reported benefit from 12 weeks of combined resistance and aerobic training in postmenopausal women with vasomotor symptoms. Kurc et al. fits that direction, but it does not settle which exercise modality or delivery model should be treated as best.
App Delivery Looked Comparable, but Dose Tracking Was Missing
The face-to-face vs. web-based comparison is the headline temptation. Most between-delivery effect sizes were negligible to small:
- Depression: BDI face-to-face vs. web-based d = 0.28.
- Fatigue: FSS face-to-face vs. web-based d = 0.20.
- Sleep quality: PSQI face-to-face vs. web-based d = 0.15.
- Predicted fitness: VO2max face-to-face vs. web-based d = 0.23.
- Muscle mass: face-to-face vs. web-based d = 0.00.
Those numbers support app-based exercise as a credible access option, especially for women limited by transportation, scheduling, cost, fatigue, or low confidence. They do not prove true equivalence.
All face-to-face participants attended the 4 supervised sessions, but neither group had session-by-session home exercise logs. The app platform’s usage records were not available after the study period, so the investigators could not verify whether the web-based group completed the same exercise volume as the supervised group.
Clinical implication: app delivery is most defensible when the alternative is no structured program, not when a patient clearly needs hands-on supervision for safety, technique, progressive loading, pain, balance risk, or accountability.
Body Fat Did Not Separate the Groups
Body-composition results were more modest than the symptom results. Body fat percentage fell within all 3 groups, including education control, and between-group effects were negligible. Muscle mass increased by about 0.16 kg in both exercise groups while the control group decreased by 0.23 kg, producing small exercise effects vs. control.
Predicted VO2max improved by 0.87 ml/kg/min with face-to-face exercise and 0.65 ml/kg/min with web-based exercise, while control changed by −0.03. Effect sizes vs. control were large, but the investigators noted that the absolute gains may fall within day-to-day variability for submaximal treadmill estimation.
Gould et al. and Baker et al. have both described body-composition and exercise-metabolism changes around menopause. Kurc et al. adds a practical point: 8 weeks may be enough to move symptoms, sleep, fatigue, and perceived quality of life before it creates a clean body-fat signal.
Practical Read: Use the App When Access Is the Barrier
The trial supports a pragmatic sequence for early postmenopause: start with a structured combined program, then choose delivery format around access, safety, and adherence.
- Best app fit: women who can follow video instructions safely, have no major contraindication to exercise, and mainly need scheduling flexibility.
- Best supervision fit: women with pain, balance limitations, low exercise confidence, technique uncertainty, or medical complexity.
- Outcome targets: depression symptoms, fatigue, sleep quality, menopause symptom burden, and quality of life may shift before body fat changes clearly separate from control.
- Tracking requirement: any real-world program should log sessions, minutes, perceived exertion, and symptom changes because this trial’s biggest comparability gap was adherence measurement.
For now, the data favor structured exercise over education alone. If forced to choose between no program and a well-designed app program, the app is a reasonable starting point. If supervision is available and needed, face-to-face delivery still has a role.
Questions About Web-Based Exercise After Menopause
Did the app outperform face-to-face exercise?
No. Web-based exercise had the clearest corrected depression result vs. education control, but most direct web vs. face-to-face effect sizes were negligible to small. The trial is better read as support for app-based access, not proof that apps are superior.
Was this a depression treatment trial?
No. The trial measured depressive symptoms with the Beck Depression Inventory in early postmenopausal women. It did not enroll women because they had diagnosed major depressive disorder, and it should not replace depression-specific care when symptoms are severe or persistent.
What exercise did participants actually do?
Both exercise groups used the same 8-week program: brisk walking plus resistance, core stabilization, and balance exercises, 3 days per week. The delivery method differed; the exercise prescription did not.
What is the biggest limitation for using this result?
Adherence tracking. The trial could not retrieve app usage records and did not collect home exercise logs, so similar outcomes do not prove that both groups completed the same dose of exercise.
References
- Kurc D, Tunali Van Den Berg AN. Effectiveness of face-to-face and web-based exercise programs on health outcomes in early postmenopausal women: a randomized trial. BMC Women’s Health. 2026. https://doi.org/10.1186/s12905-026-04457-4
- Money A, MacKenzie A, Norman G, et al. The impact of physical activity and exercise interventions on symptoms for women experiencing menopause: overview of reviews. BMC Women’s Health. 2024;24:399. https://doi.org/10.1186/s12905-024-03243-4
- Yilmaz Babacan G, Guler Cekic S, Candan Algun Z, Durmusoglu AF. Effects of exercise training on vasomotor symptoms and quality of life in postmenopausal women: a randomized controlled trial. BMC Women’s Health. 2025;25:612. https://doi.org/10.1186/s12905-025-04231-y
- Baker FC, de Zambotti M, Colrain IM, Bei B. Sleep problems during the menopausal transition: prevalence, impact, and management challenges. Nature and Science of Sleep. 2018;10:73–95. https://doi.org/10.2147/NSS.S125807
- Gould LM, Gordon AN, Cabre HE, et al. Metabolic effects of menopause: a cross-sectional characterization of body composition and exercise metabolism. Menopause. 2022;29(4):377–389. https://doi.org/10.1097/GME.0000000000001932
- Baker PA, Moore SR, Smith-Ryan AE. Physiological alterations around the menopause transition: a 2-year follow-up in PRE, PERI, and POST menopause females. Clinical Physiology and Functional Imaging. 2025;45:e70011. https://doi.org/10.1111/cpf.70011
Leave a Reply